|
farms |

|
|
Ill Fares the Land
by
W.W. Yellowlees, MC, FRCGP (Dr. Walter Yellowlees)
General Practitioner, Aberfeldy, Perthshire

The James MacKenzie Lecture, 1978
Journal of the Royal College of General Practitioners, 1979, 29, pp. 7-21.
I am grateful for the great honour the College has done me in inviting me to give this lecture. It is an honour which I neither dreamed of having, nor, knowing my own shortcomings, thought I deserved. I can, however, make one geographical claim to be a Mackenzie lecturer. Mackenzie's mother, Jean Campbell Menzies, is said to have come from a family which farmed land near the village of Amulree not far from Aberfeldy: and my brother Dave's farm of Muirhall, near Scone, on the outskirts of Perth, shares a common boundary with Pictstonhill Farm where Mackenzie was born and brought up.
Parents and family
One August day, when the fields were yellow with ripening corn, in search of inspiration for this lecture I crossed the fence to look on Mackenzie's birthplace. The old stone cottage is now much dwarfed by new buildings and altered by the needs of modern agriculture. Like Professor Alex Mair, whose splendid biography of James Mackenzie (Mair, 1973) is such a boon to Mackenzie lecturers, I marvelled at the thought of the family of four boys and three girls reared in this small cottage with its hundred acres of land.
As I looked on those fields and hills, I thought of men like James Mackenzie, nurtured in those Victorian days amid the unceasing toll of wresting a living from the land. The Scottish presbyterian tradition of family worship, Bible study, and strict observance of the Sabbath, was ingrained in their young lives. However much the strictness of these observances in childhood may have led Mackenzie and others of his generation to reject institutional religion altogether in later life, it is clear that his enquiring mind was powered by a strong spiritual force, and although he did not suffer fools gladly, his outgoing and warm-hearted personality stemmed from the faith and the tradition in which he was reared.
His father, a progressive farmer ahead of his time, was the first in the district to reduce the hours worked by his farm servants from the accepted norm of 10 to 12 hours to nine hours a day, and the Pictstonhill farm servants did not often leave. His mother had a strong, indomitable spirit and it was often first to her that the villagers turned when in need. In this background we can see the sources whence sprang Mackenzie's strength of character and his single-minded application to research amid all the distractions and frustrations of general practice. The story of the struggles and triumph of that research is well known and is one of the most remarkable achievements in the annals of medicine.The search for prevention
However, Mackenzie was a man with an unfulfilled mission, and even after he had established himself as one of London's leading consultants, with a tremendous reputation and a huge income for those days of £8,000, he was restless and dissatisfied. He was searching for better understanding of the origins of disease and for prevention; he had become convinced that in this search the medicine of the hospital and of the specialist, which he had experienced for 11 years, was going in the wrong direction. "I am convinced," he wrote (Mackenzie, 1919), "that the conception of specialism dominant today is wrong, and helpful as this specialism has been in many ways, nevertheless, instead of enlightening it tends to darken our understanding in a cloud of detail." "The modern conception of specialism is responsible for much confused thinking and so for the delay in the attainment of knowledge" (Mackenzie, 1926).
General practice, argued Mackenzie, was the place to understand the origins of disease.
"If the conditions which predispose to or provoke disease are to be recognised the investigator must have the opportunity of seeking the circumstances which led up to the invasion of the disease" (Wilson, 1927).
In repeating Mackenzie's stricture on specialism I imply no criticism at all of the devotion and skill of those consultants with whom, during 30 years of general practice, it has been my privilege to work. Increase in knowledge and in the scope of medical technology have made more specialization in the delivery of medical care inevitable. In general practice we could not exist without specialist support.
But for those following Mackenzie who seek to understand the origins of disease and the basis of health I believe his words ring true today: "The modern conception of specialism is responsible for much confused thinking".Institute of Clinical Research, St Andrew's
Mackenzie hoped that with better training in the investigation of the earliest signs or symptoms of disease an enlightened band of general practitioners might learn to avert later manifestations. So, at the age of 65, in spite of increasing attacks of angina, undaunted in his search for prevention he turned his back on Harley Street and in 1918 returned to general practice. Few understood what he was doing: some thought he was crazy.
In his broad approach to the problems of health and disease he was far ahead of his time. But he did not know (what I believe is blatantly obvious today) that the skills and ways of prevention are utterly removed from those of cure. He did not know that health cannot be created by studying even the earliest symptoms of disease, nor by medical intervention, however skilled, or however well organised. As a project for prevention the Institute of Clinical Research which he founded at St Andrew's was thus doomed to failure. But the fallacy that early diagnosis and various screening programmes will make us healthier dies hard and remains the priority today for some enthusiasts for prevention.The rising tide of morbidity
To understand this fallacy we need only study the record. General practice has indeed developed along the lines advocated by Mackenzie. We have today vastly improved methods of recording and opportunities of studying these early symptoms which he thought so important. The part of our gross national product devoted to all medical services has increased from 3.8 per cent in 1951 to 5.7 per cent in 1975.
We have more doctors per head of the population than ever before but, alas, all this increased expenditure of money and improvement in skill appears to have made very little difference to the general health of the nation.
Success in combating infection has been impressive, but during the twentieth century there has been a rising tide of new diseases whose ravages continue at a high level among people of industrial societies.
In 1918, when Mackenzie left London for St Andrew's, coronary thrombosis was virtually unknown (Michaels, 1966); so was diverticular disease of the colon (Painter and Burkitt, 1971). Both are now among the commonest diseases seen in practice today. The decay of our arteries as seen in coronary thrombosis is matched by the continuing incompetence of our veins; about 10 per cent of the population have varicose veins (Cleave, 1960) and many sufferers are greatly incapacitated by their complications.
Duodenal ulcer, which at the beginning of the century was very rare (Illingworth, 1953), remains a common, crippling abdominal disease. The arthropathies and rheumatic complaints continue to cause disability on a vast scale (Wood, 1971).
Since the closing decades of the last century there has been a real increase in gallbladder disease (Heaton, 1972), appendicitis (Burkitt, 1971) and diabetes (Cleave, 1956). Recent evidence from Glasgow appears to show a considerable increase in diabetes in children (Craig et al., 1977).
In Scotland, so terrible is the state of the nation's teeth that 44 per cent of adults aged 16 and over have no teeth at all (Todd and Whitworth, 1974).
The worst of all our afflictions is cancer. Since 1930 there has been a 62 per cent increase in Scotland's crude mortality rate for cancer which then standardised gives an increase of 15 per cent (DHSS, 1977).
In a survey of 25 countries Scotland had the highest mortality rate for cancer in men and the fourth highest for women (Kemp and Ruthven, 1978).
Table 1. Cancer in one rural practice
(population -- approx. 3,500).1975 1976 1977 Total Number of patients 17 17 17 51 Average age of patients 70 Number of patients under 70 22 Number of patients under 60 11
In our Aberfeldy practice we have diagnosed 51 new cases of cancer in the last three years (Table 1). In noting this high incidence in such a small community we must remember that like most rural practices ours is heavily loaded with elderly people: 23.6 per cent of our practice population are over 65, but 43 per cent of our patients with cancer were under 70, and 21 per cent were under 60. A look at the site of these cancers shows a heavy ponderance of bowel cancer (Table 2).
Table 2. Sites of cancers in one rural practice (population -- approx 3,500) Colon -- 12
Rectum -- 315 Pharynx 1 Prostate 1 Abdominal* 2 Mouth 1 Lung 5 Antrum 1 Skin 5 Oesophagus 1 Breast 4 Kidney 1 Ovary 2 Brain 1 Cervix 2 Osteogenic sarcoma 1 Stomach 2 Lymphosarcoma 1 Bladder 2 Lymphatic leukaemia 1 Larynx 2 Total 51 *Site of primary growth not known
This preponderance does not agree with the Scottish Home and Health Department's statement (1977) that cancer of the colon is the third commonest cancer in Scotland following that of lung and stomach. Probably this discrepancy reflects our population's age group and maybe these last three years show an atypical wave of incidence. Unfortunately, we do not have accurate figures for previous years.
I believe it is true to say that in those countries which have achieved unparalleled advance in technological skill in medicine and in what is called standard of living we are witnessing the decay of man -- the decay of his teeth, his arteries, his bowels, and his joints on a colossal and unprecedented scale.
We cannot blame it all on the ageing of the population. Many of the modern forms of decay afflict young and old and when we look at the record of the working male population it seems equally depressing.
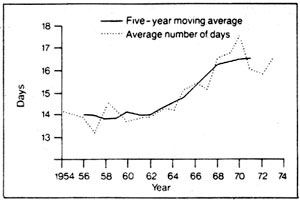
Figure 1 shows the annual number of days of incapacity per insured person from 1953 to 1973. The commonest diagnosis was bronchitis followed by diseases of the circulatory system; rheumatism, and arthritis came third. It would seem that the launching of the Health Service in 1948 brought no improvement at all in the capacity of employees for work: indeed the opposite was the case. Even if the graph expresses only changing attitudes or lack of job satisfaction, it does seem to demonstrate an ever-increasing load on the nation's medical and social security services.
Figure 1. Average number of days of incapacity per insured person per year (1953/14 to 1972/3).
Source: Office of Health Economics (1975).
If a rising standard of living and ever more sophisticated medical care have failed to stem the twentieth century's epidemic of new disease and disability, where do we go for prevention? It is my aim in this lecture to provide the answer.
False hopes of health
First, however, I want to comment on the delusion which led to the establishment of the wrongly named 'National Health Service', the delusion being that if only everyone had unfettered access to the best available medical services, people would get healthier.
By the turn of the century medical scientists had seen in the work of Pasteur, Lister, Koch, Simpson, and others new worlds of opportunity in medicine and in surgery. They felt confident in expecting all the answers to the problems of prevention as well as of treatment from advances in medical research.
In wider fields of thought also, the supremacy of science had become the new hope of mankind. Those who followed Darwin saw man not as part of God's image and of an awesome and mysterious Divine purpose, but merely as an evolved ape, a bag of haphazard molecules. The writings of Freud and Karl Marx further widened the growing gap between science and established religion. No need was there now for the wonder or for reverence; budding scientists embraced the idea, held deeply in the human psyche since the Garden of Eden, that man was far smarter than nature.
So, in the euphoria following Hitler's war, politicians and people eagerly accepted Sir William Beveridge's Welfare State with its National Health Service in the naive belief that they were banishing forever the spectres of disease and hunger.The Organic School and Sir Robert McCarrison
Not all observers in the 1940s shared in the false hope of health through a comprehensive medical service. The writers of what is sometimes called the Organic School, whose most forthright and eloquent leader was Lady Eve Balfour (Balfour, 1948), shared a common theme; human health could be understood only in the context of vital relationships between man and the living world of soil, plant, and animal. They emphasised that our ignorance was far greater than our knowledge but that we already knew enough to predict that if the disruption of those natural relationships by new technologies in agriculture and food processing continued, search for health by medical advance would be in vain -- our bodies would inevitably decay. This conclusion followed the research of one of the best known of the early pioneers in the new knowledge of nutrition, Sir Robert McCarrison.
McCarrison joined the Indian Medical Service in 1901 and as a young officer soon made his mark by original research into the cause of sandfly fever (McCarrison, (1906, 1908). He became well known for his publications on goitre and deficiency diseases (McCarrison, 1917, 1921), In his early years in the Northern Frontier region, in a role similar to that of general practitioner, he was deeply impressed by the health and vigour of certain races there, notably the Sikhs and the Hunzas: they suffered from none of the major diseases of the Western nations such as cancer, peptic ulcer, appendicitis, and dental decay. They were long lived and their vibrant health was in marked contrast to the high morbidity of other races in the southern part of India.
Here was a control group of human beings with a near zero incidence of morbidity; McCarrison realised that in this phenomenon he was observing something of unique importance in human affairs.
As Director of Nutrition Research in India he later confirmed in a long programme of research that the absence of morbidity he had witnessed was not due to any accident of race or climate but simply to sound nutrition.
Colonies of rats fed on food identical to that of those Northern races constantly showed all the signs of health; he was thus able to maintain a control colony of healthy stock animals which repeated long-term feeding trials contrasted with the poor physique, widespread respiratory infections and gastro-intestinal degeneration suffered by rat colonies fed on food identical to that of the poorer people of Madras and Bengal. A high incidence of infection and degeneration was also noted in rats fed on a typical poor class British diet of tinned meat, boiled potatoes and cabbages, white bread, margarine and jam, and much sweetened tea (McCarrison 1953).
Food for health
The qualities of the control diet as eaten by the healthy Northerners were as follows:
- It was grown by people who were devoted and expert farmers, maintaining the fertility of their soils by organic methods.
- The bulk of their carbohydrates was in the form of wholegrain cereals; they ate no white flour and little or no sugar.
- Much of their protein and fat came from an abundance of milk and milk products such as butter and cheese. Meat was taken occasionally about once a week.
- This basic ration was supplemented by a wide variety of fruit and vegetables, often eaten raw.
- Breast feeding was universal.
McCarrison was not able to identify which particular disease was caused by which particular dietary fault or deficiency. In his approach to health as a whole, fragmentation of knowledge was at this stage neither possible nor necessary.
What mattered was the whole diet and its effect on the whole organism and the need of mankind for food which was varied, fresh, unrefined, and free from artificial additives. Without such food McCarrison repeatedly demonstrated that growth and stature were substandard, and resistance both to infection and degeneration lowered; this appeared to be true for some types of the worst of all degenerations -- cancer.The fence or the ambulance
In a review of McCarrison's work Wrench (1938) emphasised its revolutionary message; of all factors which make for human health the greatest single factor is adequate nutrition. This simply means that however excellent are housing, clothing, sanitation, exercise performance, or smoking habits, inadequate nutrition such as still prevails in Britain today will continue to cause widespread disease.
A summary of McCarrison's work and conclusions published in the British Medical Journal in 1936 was greeted by a deafening silence. [See Nutrition in Health and Disease.] Yet here was the answer to our question, "Where do we go for prevention?" But our profession, forever darkening their understanding in Mackenzie's cloud of detail, were too busy studying disease to pay any attention to this signpost to health. The sulphonamides had just been discovered, which helped to confirm the faith of specialism in health through new wonder drugs and new medical techniques.
Maybe it was unfortunate that the publication of McCarrison's summing up came at the same time as the chemotherapeutic breakthrough. Now that an agent had been discovered which would inhibit invading pyogenic bacteria without too much damage to the host, the study of disease became much more exciting. By their training and attitudes doctors were not attuned to believing that such a subtle measure as dietary reform could prevent many of the diseases which they daily encountered. Their failure in this respect was dramatized in a little poem which appeared in the Soil Association Journal 25 years ago (Malines, 1953):
'Twas a dangerous cliff, as they freely confessed,
Though to walk near it's crest was so pleasant,
But over its terrible edge there had slipped
A duke and many a peasant;
So the people said something would have to be done.
But their projects did not all tally:
Some said, "Put a fence round the edge of the cliff";
Some, "An ambulance down in the valley".
But the cry for the ambulance carried the day,
For it spread to the neighbouring city;
A fence may be useful or not, it is true,
But each heart became brimful of pity
For those who had slipped o'er that dangerous cliff
And the dwellers in highway and alley
Gave pounds or gave pence, not to put up a fence
But an ambulance down in the valley.
"For the cliff is all right if you're careful," they said;
"And if folks even slip or are dropping,
It isn't the slipping that hurts them so much
As the shock down below -- when they're stopping."
So day after day when these mishaps occurred,
Quick forth would the rescuers sally,
To pick up the victims who fell off the cliff
With their ambulance down in the valley.
The response of the profession and government to the ravages of new disease has been to call for more ambulances. But as the cost of new sophisticated models is prohibitive, and as the nation faces bankruptcy, at last our thoughts are turning to the need for fence building. There seems to be, however, no agreement by professional spokesmen as to how to go about it.New evidence of the role of nutrition
The failure so far by profession and people to grasp the true nature of the fence seems all the more surprising as newer research in nutrition repeatedly confirms McCarrison's thesis.
I have selected under the following four headings some observations which further confirm my belief in the all-important role of nutrition in prevention:
- Morbidity in rural practice
- Lessons from primitives
- The researches of T L Cleave
- McKeown's study of population.
1. Morbidity in rural practice
As a newcomer to rural practice in 1948, while visiting families at their mealtimes I realised with horror that in this lovely, fertile Highland valley my patients were eating food very little different from that which had had such a devastating effect on McCarrison's rats.
The main feature of the modern Highlander's diet is the absence of fresh vegetables and salads, the absence of wholegrain cereals, and the massive intake of refined carbohydrates. Porridge no longer adorns the breakfast table, and the Scottish high tea of scones, cakes, biscuits and tinned jam is a festival of sugar and starch.
I thought it surprising that farmers who devoted their lives to rearing healthy farm animals by sound nutrition should allow their wives to load the kitchen table with processed trash. If the teeth of their cattle were to rot as badly as did those of their children they would have taken strenuous measures for prevention. But agriculture seemed no longer to be thought of as a process for feeding people -- it had become another industry modelled on the factory production line. The balance sheet according to bogus monetary values was all that mattered. Human health was forgotten.
I became convinced that here, in Mackenzie's words, I was seeing the "condition which led to the invasion of the disease". Here was the reason why our practice, so far removed from any kind of urban stress, had such a high incidence of diseases like peptic ulcer, coronary heart disease, hypertension and cancer; and why even in the clean Highland air, recurring respiratory infections were relatively common. The quiet rural life and employment involving hard, physical work seemed to give no protection at all against diseases supposed to be due to lack of exercise and urban-type stress. For instance, duodenal ulcer, supposed to be a stress disease, appeared to be common; in the last three years we have averaged six new cases annually.
The most likely explanation for the awful human decay I was witnessing was the kind of food I had described food which McCarrison had shown to be associated with widespread disease; and how tragic that nowhere in all Britain could a control population be found.2. Lessons from primitives
Control populations are becoming rare as ramifying trade routes carry the processed foods of the West to even the remotest human settlements.
The contrast in disease patterns between primitives and moderns which so strikingly confirms McCarrison's experience was well researched by Price in the 1930s (Price, 1945).
Post-war publications tell of the same contrast among many different races (Schaefer, 1959; Stefanson, 1960; Cleave et al., 1969; Burkitt, 1973; Cleave, 1974).
One of these, a fascinating essay in the Journal of the Women's Medical Federation by a general practitioner, Dr Mary Jackson (1956), describes the rising incidence of dental decay, obesity, coronary disease, diabetes, and pregnancy toxaemia which she observed among the Canadian Metis Indians after a new road to northern oil fields brought to those hunters and gatherers the processed foods of civilisation.
In the British Isles no 'primitives' are left; indeed, with the total destruction of rural economy everywhere in our island, primitives, if communities in the more isolated rural areas deserve that name, are more dependent on processed foods than are Londoners.
A recent example is one of my patients with a cluster of diseases often seen in those employed in rural occupations. He was a 61-year-old gamekeeper who had no teeth of his own, a history of coronary artery disease, a duodenal ulcer, and had suffered a left-sided stroke which ended his working life. His case is typical of many a Highlander.
There now seems to be no evidence that in Britain rural populations enjoy better health than town populations. But the far better health and stature of the higher social classes (Health Departments, 1976) is, in my opinion, yet further confirmation of McCarrison's thesis.
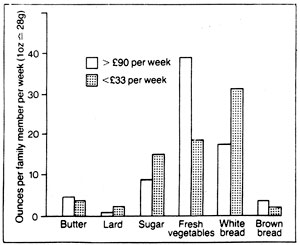
The higher income groups eat less refined carbohydrate and more fresh green food than the lower income groups, which is certainly the impression of mealtime visits; the National Food Surveys seem to agree (Figure 2).3. The researches of T L Cleave
Renewed interest in the last 20 years in the epidemiology of diseases of civilisation has been due, above all, to the work of Surgeon Captain T L Cleave who, like William Harvey and John Hunter, brought to the study of medicine the flair of a naturalist. Cleave elaborated the adverse effect of one feature of the food of industrial societies noted by McCarrison -- their dependence on refined carbohydrates. In the 1930s he observed the relief of constipation when the fibre of wheat flour which had been removed in milling was restored to food in the form of unprocessed bran (Cleave, 1941). Such was the success of this simple measure during the last war that there was unrest among the crew of the battleship King George V when the supply of bran failed (Cleave, 1974). (How could Britannia rule the waves if her bowels were hopelessly constipated?)
Figure 2. Family food consumption by wages of household. Source: National Food Survey, 1976, using household comprising two adults and two children (Clayton, 1978).
In digressing briefly to ask why industrial peoples substitute in place of wholewheat flour (which is so simple to mill and pleasant to eat) a white, inert, tasteless, constipating powder, robbed by complex processing of most of its fibre and much of its virtue, we learn as much of man's psyche as of his nutritional needs.
From early history sifted white flour was equated with wealth and status, coarse wholewheat with the rough inferior peasant.
In England the physicians of the seventeenth century noted that white flour was constipating and fattening, wholewheat laxative and slimming (McCance, 1956). They were quite right (Heaton, 1973). But by the eighteenth century to have white wheaten bread on the table was a symbol of wealth and class. So the servant classes and the city poor clamoured to be up with the Jones's (McCance, 1956). By the beginning of the nineteenth century all classes were eating white bread, and by 1865 it became more profitable for the millers to make white flour, so everyone was happy and thus was laid the foundation of the constipated state.
Cleave pointed out that the effect of partial removal of fibre in the milling process in the case of white flour was compounded by its complete removal by refining, in the case of refined sugar. Moreover increasing consumption of sugar displaced natural fibre-containing foods, thus aggravating the cause of constipation with its complications of diverticular disease, haemorrhoids, varicose veins, and large bowel cancer.
After his appointment in 1955 as Director of Medical Research at the Royal Naval Medical School, Gosport, Cleave continued his researches on the effect of different organs and tissues of diets high in refined carbohydrate (Cleave, 1960, 1962, 1969). He gave the concept of a single "saccharine disease" having, like syphillis, a remarkably widespread pathology, but one simple cause.
One mechanism elaborated by Cleave sheds light on the total confusion arising from conflicting theories of the dietary cause of coronary thrombosis. This mechanism is over-consumption caused by abnormally swift and massive absorption of carbohydrates when the carbohydrate has been unnaturally concentrated -- in the case of white flour by 30 per cent and in the case of sugar by almost 100 per cent.
According to this theory the abnormally swift absorption of refined sugar by disrupting normal glucose tolerance in time leads to the onset of diabetes, thus explaining the high incidence of this disease in advanced countries, its absence in primitives, and its recent explosive increase in parts of Africa (Cleave, 1974).
In people eating large quantities of refined sugar, 40.5kg (90 lbs) a year, the constant appearance together of obesity and, after a latent period of at least two decades, diabetes and coronary thrombosis, argues a common cause. Exactly how abnormalities of carbohydrate absorption and metabolism damage our arteries are not yet known. Professor John Yudkin has emphasised the importance of hormone imbalance resulting from hyperinsulinism and changes in corticosteroid output which in some people follows a high consumption of sugar (Yudkin, 1972).
Surveys in this country, which appear to show no greater incidence of coronary thrombosis among subjects with an intake of sugar apparently higher than controls (Lancet, 1970), suffer from a fatal weakness -- the absence of true controls, eating little or no sugar. Only populations who over a span of 30 years or more have had minimal sugar consumption, say in the region of 9 to 13.5kg (20 to 30 lbs) per head annually (a level which prevailed in the first half of the nineteenth century) could be regarded as true controls. Such groups would be impossible to find today in Britain. Teenage children are eating about 210g (7.5 ozs) daily (Yudkin, 1972) and much of our sugar is consumed as food additive (Jukes, 1977).
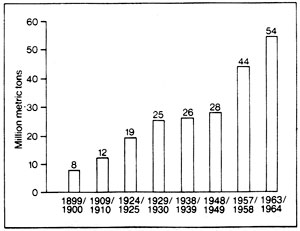
Figure 3. World sugar production (1899/1900 to 1963/4). Source Ackroyd (1967).
The huge increase in sugar consumption throughout the world (Figure 3) coupled with the replacement of wholegrain cereals by refined flour will result, if Cleave's theory is correct, in the ever-widening spread of those diseases enumerated by him.4. McKeown's study of population
Recently, McKeown has argued powerfully that the trebling of the population in Britain from 1700 to the mid-1800s was due not to better medical care or improved hygiene but simply to a fall in mortality resulting from better nutrition (McKeown, 1976).
The second agricultural revolution of the eighteenth century greatly increased the supply of our home-grown food. McKeown's account of increased resistance to disease from improved nutrition agrees absolutely with McCarrison's thesis.
It is of the utmost importance to note that the trebling of the population, thanks to increased food production, occurred before the introduction of chemical fertilizers.Chemicals, or farmyard manure
This fact casts doubt on the popular belief that a hungry world cannot be fed without massive application of soluble chemicals to the soil. This subject seemed to me so important that over three years in my garden I have tried to find out what happens when you grow food without using either chemical fertilizers or toxic sprays.
Ten years ago the rough sloping stone-strewn ground around our new house had to be levelled and terraced to make two small vegetable plots. Only composts made from cow or poultry dung, with the addition of quite a lot of human urine, were used as fertilizer. Our winters are hard and the growing season relatively short; but the response of unpromising land to this treatment seemed so generous that in order to measure our output we weighed all our crop from 1 April 1977 to 31 March 1978 (Table 3). Tomatoes and cucumbers from two small greenhouses were added. The weight of food was over 510kg (half a ton) and if the greenhouse crops are excluded is at the rate of over five tons to the acre.
Faith in organic methods is confirmed by work in Holland, France, and England which shows that output from organic farms can be similar to those using conventional fertilizers (Hodges, 1978). Even if in some circumstances crop yields can be increased by the use of chemicals, we are largely ignorant of what chemical methods do to the health of the consumer. Several published results have shown a measurable change in nutritional quality when chemicals are used in place of organic manures (McCarrison, 1926; Rowlands and Wilkinson, 1930; Schuphan, 1974).
These results may be questioned but there is no doubt at all of the fact that only a small proportion, probably about one fifth, of chemical fertilizer put on the land is actually taken up by the crop (Milton, 1975). Much of the remainder is leached out into our surface water systems where rising nitrate levels in some areas are causing concern; there is evidence which suggests that high nitrate levels in drinking water and crops can be a cause of stomach cancer (Lancet, 1977).
Table 3. Food produced from a small garden
-- 1 April 1977 to 31 March 1978.Area 310 m2 (371 sq. yds) Glass (two small greenhouses) 19m2 (23sq. yds) Total 329 m2 (394 sq. yds) Potatoes 194 kg (430 lb) Tomatoes 81 kg (181 lb) Lettuce 39 kg (86 lb) Peas and beans 37 kg (81 lb) Courgettes 35 kg (78 lb) Onions 34 kg (75 lb) Brassicas 33 kg (74 lb) Strawberries 27 kg (60 lb) Beetroot 23 kg (52 lb) Parsnips 19 kg (43 lb) Leeks 14 kg (30 lb) Carrots 9 kg (20 lb) Other soft fruit and vegetables 41 kg (91 lb) Total 586 kg (1301 lb)
Discussion on this subject is incomplete without looking at the traffic on the great estuaries of Britain, on which boats or barges laden with sewage sludge going seawards pass incoming boats loaded with artificial fertilizer. Millions of tons of the sludge containing potash and phosphate are daily dumped at the mouths of the estuaries where it fouls up the seas and the shores. The fertilizer, imported to the detriment of our balance of payments, is dumped on the land where in its turn it fouls up the inland waterways (Wylie, 1959). Both processes will in the long run, I believe, hasten the progress of human decay.
To sum up so far: the researches of McCarrison, Cleave, and many others, and our observations in practice all teach the same lesson that the way to true prevention is by sound nutrition. Without adequate food all other measures will be of little avail.Nature's laws
However, as the organic school has for long pleaded, sound nutrition is much more than counting calories or adding up inert vitamins, minerals, and proteins. It is part of a living process, embracing man's relationship with the plant and animal world and is subject to nature's laws.
An understanding of these laws comes as much from inbred wisdom as from advanced degrees in biochemistry. Mackenzie knew this; his mind was searching along the way of ecology when he wrote, "An increase in the knowledge of natural laws leads to simplification" (Mackenzie, 1919).
The simplicity of the idea that so much disease could be caused by modern malnutrition may be difficult to accept, and the thought of nature's laws quite baffling. Man bestrides a natural world. He dominates all living things but he is utterly dependent on them. He is supported by the plants, the trees, and the animals. The whole system rests on the soil which is itself vibrant with life. If any part of the supporting system is taken away, man will begin to fall off his perch.
The whole system is powered by energy from the sun, and the moon reminds us of the unfortunate propensity of man for lunacy. By lunacy I do not mean that which afflicts the occupants of the 125,000 mental hospital beds in Britain. I mean his tendency to infantile behaviour, to embrace and act out irrational beliefs and idiotic ideas. This form of lunacy from time to time afflicts us all and is a condition from which no social class or group, however privileged or academic, is entirely free.
The laws of nature applied to nutrition simply require that the flow of nutrients from the soil through the plants and the animals to man should be as little meddled with as possible. The flow is dependent on an infinite number of biological relationships which can neither be counted nor measured.
There are, of course, soil scientists, botanists, zoologists, anthropologists, and others who can measure and analyse little separate bits of the system. Inevitably they are steeped in specialism and vast libraries are filled to overflowing with their findings -- a huge store of knowledge which for the unwise is apt to become a dense cloud of detail, obscuring simple truths.
Minimal cooking is a blessing which has added greatly to our delight in food. Used sparingly and judiciously it can surely do us no harm. But what is the effect of manmade chemicals, added to all parts of the food chain -- especially to food which has been subjected to repeated cooking and other forms of fabrication?
In Britain one estimate gives a weight of 1.44kg (3.2 lbs) of chemical additive consumed per head of the population annually -- that is equivalent to 12 aspirin-size tablets daily (Thomson, 1975). No food technologists, however erudite, could possibly predict the long-term effect of this chemical onslaught on our metabolism, nor say that it has not played a part in the cause of our high incidence of cancer.
The separation of urban populations from the world of nature and the intensification of specialism in biological research has led to the spread of beliefs on prevention which show no understanding at all of nature's laws.
At a time of ever-increasing centralization of government control there is grave danger of such beliefs being enshrined as dogma and incorporated in programmes for prevention, of unproven value and of possible danger.The dogma of animal fat
This danger is well illustrated by the dogma of animal fat and the branding of animal fat as the villain of human nutrition.
Animal fat has been an important part of human diet since our ancestors came down from the trees and started hunting and, even more important, since they learned to domesticate wild animals 10,000 years ago.
It is, therefore, not surprising that some populations who by our standards eat enormous quantities of such fat have in their natural habitat no coronary disease at all (British Medical Journal, 1971; Mann et al, 1964). Their freedom is not, I believe, due to their habit of physical exercise; in my experience the relatively hard physical work of rural occupations is no protection from coronary disease.
The freedom from coronary thrombosis in groups eating large quantities of animal fat is well demonstrated by complete absence of any description of acute infarction in Mackenzie's writings.
Mair (1973) mentions "the failure by him and others of his era to recognise the significance even the presence of that condition so prominent today -- coronary thrombosis or myocardial infarction" (my italics).
It is inconceivable that men of Mackenzie's diagnostic skill would have failed to recognise myocardial infarction had it occurred in their day as it does now. Dr Jack Henderson, my respected erstwhile neighbour from Pitlochry, in his Mackenzie Lecture of 1964 stated: "In 1925 coronary artery thrombosis was a rare disease and I do not recall seeing even one example of it when I was a student".
The failure of Mackenzie and his contemporaries to recognise acute infarction was simply because it was not there. Michaels (1966) has traced the history of coronary disease from the first record of angina in the eighteenth century and has confirmed the absence of acute infarction until the present century. But in Mackenzie's day the Victorian and Edwardian servant-keeping classes, that is, almost one-third of the population of England and Wales, ate as much or more animal fat than is being eaten today. And they were physically lazy (Michaels, 1966).
There has been no increase in fat consumption which could possibly explain the onset of coronary thrombosis in the 1920s and its explosive increase in post-war years (Trenchard, 1977).
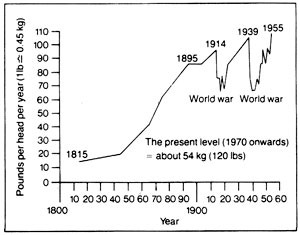
This record of fat consumption may be contrasted with the huge increase in the consumption of sugar which has occurred over the last 150 years in Great Britain (Figure 4).
Figure 4. The rise in sugar consumption in the UK from 1815 to 1955. Source: Cleave (1974).
Obsession with blood cholesterol levels has led to some extraordinary dietary cults. These would have us substitute margarine for butter, restrict our egg consumption to three a week, and make the taking of cream a sin (Connor and Connor, 1972). (Whoever heard of anything so absurd as strawberries and skimmed milk?)
A recent suggestion that high blood cholesterol may simply be the expression of a bodily defence mechanism designed by nature to repair arterial damage in my opinion gives a better explanation of the facts than any other (Kaunitz, 1977).
Hypercholesterolaemia would (according to this explanation) have nothing to do with the cause of atheroma but could be compared to the high white cell counts which occur in chronic infection. It would thus be as absurd to blame high blood cholesterol as the cause of arterial disease as to blame white cell counts as the cause of chronic infection.
The popular belief in the efficacy of increasing the ratio of polyunsaturated dietary fat as a means of preventing coronary disease finds no confirmation at all in those populations who have succeeded in increasing greatly the proportion of vegetable oils in their food and yet have experienced a steep rise in the incidence of coronary thrombosis (Antar et al., 1964; McMichael, 1977).
The campaign against traditional foods like eggs, butter, and milk, which McCarrison showed were such an essential part of human food has, of course, been given great impetus by the manufacturers of processed oils whose trade would flourish if housewives could be persuaded to change from butter and lard to margarine and corn oil.
Government and the food industry
The role of government in prevention is fraught with great danger and difficulty; governments should not tell citizens what they should eat or drink.
In discussing nutrition, the White Paper on Prevention and Health (DHSS, 1977) sensibly takes this view and gives the main role of government as assembling, assessing, and disseminating information. But there is the rub. What information? If it is information based on false dogma it may have the opposite effect of that intended. In the White Paper there is little evidence of an awareness of the conflict which I have tried to highlight -- the conflict between the trading interests of those who manufacture food or chemicals and the needs of human health.
The urgent need to look at how we are being carried along by the food industry has been well described by Professor Ross Hume Hall of McMaster University, Ontario, who has drawn attention to the following prediction by a spokesman of General Foods Incorporated of America (Hall, 1978):
"We are moving gradually into a world of designed consumer foods. Natural farm produce such as milk, potatoes, and grains are no longer just complete foods to be eaten as part of a meal. They have become ever-expanding sources of raw material to be utilized as building blocks for new and more diverse foods."
All doctors who wish to pay more than lip service to prevention should resist these trends to the utmost. General practitioners could give a strong lead in creating a loud and rising demand for fresh, whole food.
That demand could be reinforced by government action designed to start the building of the fence of prevention without infringement of individual liberty. Here are some suggestions for legislation towards dietary reform:
- Food labelling. No article of food on sale in shops should be exempt from compulsory labelling, in letters large enough to be easily read, of all artificial additives including quantities of additives.
- Food colouring. Food which requires artificial dye to make it attractive must have something wrong with it. All artificial colouring of food and drink should be banned. Such a law would do away with the extraordinary anomalies occurring in North America. Again I quote Professor Hall (1977): "Red dye number two (amaranth) causes cancer in the United States, but in crossing the border it apparently becomes so benign that it is permitted to colour about one third of all manufactured food sold in Canada. Red dye number 40 (another coal tar dye) is just the reverse, deadly in Canada, benign in the United States".
- Bread. The aim of new legislation should be to make available to all the population bread baked from freshly ground wholewheat flour. Inevitably this would necessitate much reorganisation and decentralisation of the milling and baking industries. By tax or subsidy such wholewheat bread should be cheaper to the housewife than white.
- Sugar. A substantial tax or duty should be imposed with the object of achieving a drastic cutback in the consumption of sugar. This would give an opportunity for traders and growers to substitute natural sweeteners in the form of dried or fresh fruits.
- Advertising. Misleading advertising of food should be penalised; for example, those advertisements which use images of fields and farmyards to emphasize the value of natural food in order to sell a highly processed and unnatural food, such as a brand of margarine or a bar of chocolate.
Administrative changes
Administrative changes might help to bring an end to the present Orwellian use of the word 'health' when what is meant is 'disease' or 'medical'. The health part of the Department of Health and Social Security would be renamed the Department of Medical Services and its Minister would be in charge of the National Medical Service.
A new Ministry of Land Use, Food, and Health might take on the monumental task of restoring some balance between town and country, of making Britain self-supporting in basic foods, of encouraging the consumption of fresh home-grown food rather than convenience foods.
Human health would thus be seen as the highest priority of land use; every encouragement would be given to the new marketing organisations which are expanding in Britain and in other European countries, founded by those who seek to give consumers the opportunity of buying organically grown food. A change to organic farming could not be achieved without a substantial return of population to the land and a proliferation of smaller labour-intensive units. The saving of fossil fuel energy, the redistribution of population, and the rescue of our surface water from pollution and of our food from toxic residues which would result from biological rather than chemical farming would surely in themselves make such changes in agriculture highly desirable.
These beginnings in building a strong fence would be violently opposed by the new industries which, as we have seen, are set on a course of ever more food processing and which have such vast resources for advertising their products and for influencing scientific research.
My suggestions, I am well aware, will also be greeted with derision by scientists who are missionaries for orthodox dogma.
Again I will be criticised for not mentioning in a talk on prevention the subject of tobacco or alcohol. I am sure that it is sensible to spend taxes raised in the sale of cigarettes and alcohol on warnings of the danger of addiction but to do so while ignoring far more widespread dangers of malnutrition is to mistake priorities. It is also just possible that carcinogens of tobacco might be better resisted in a well-fed population.
Heretics are for burning. But we would have no Mackenzie Lecture if the man whose memory we annually honour had not repeatedly questioned the orthodoxy of his time. His brother wrote of him, "He was thinking, devising, enquiring into the reason of things and never content with things as they are because authority said so" (Amulree, undated).
"Don't believe a word of what Mackenzie said, blot it out. He's faddist," cried a professor of medicine to his students after Mackenzie , who had demonstrated that a patient's heart murmur was quite innocent, had left the lecture theatre (Mackenzie papers).Ill fares the land
What a fragile treasure is truth! Especially when the cloud of detail is so large, the confines of specialism so small, and the sinews of propaganda so strong.
Poets often see the truth of the human condition better than scientists:
Ill fares the land to hastening ills a prey
When wealth accumulates and men decay.
Goldsmith, in The Deserted Village, certainly painted an oversentimental picture of village life in his native Ireland in the eighteenth century but he saw clearly that the strength of a nation depends on a flourishing rural economy:
But a bold peasantry their country's pride
When once destroyed can never he supplied.
The saddest thing I have had to witness in my 30 years in Aberfeldy is the relentless drain of "the bold peasantry" from the farms and estates and villages of the Upper Tay Valley, a process which has been going on so long that It has made a depopulated wilderness of much of rural Scotland. One result, and a very serious one, of this depopulation is the loss of human stock, bred and brought up close to the realities of nature -- stock of which Mackenzie's parents were shining examples.
As rural depopulation relentlessly progresses in industrialised countries, huge conurbations spread like cancers over the land so that now two thirds of all people in these countries live in and around cities (Ward, 1976).
A notable exception is Switzerland with its enviable record of stable currency and strife-free industry where only 35 per cent of the population live in cities larger than 200,000 inhabitants (Ward, 1976). It would seem from the Swiss example that flourishing industry need not create deserted villages.
How can we restore to our land pride of place to the small mixed family farm which conserves and enhances fertility and is the most highly productive unit of all (Ward, 1976; Hyams, 1976)? I do not know the answer to that question but I am sure that in the present state of the world, a nation such as ours which grows only half its own food and sees more than a million of its men standing idle in the city streets while thousands of acres stand idle in the countryside, is giving an example not of nationhood but of lunacy.
These thoughts raise burning questions about the future place in our lives of industry, technology, and agriculture. After going so far along the road of industrialism we seem, in Britain, to have come to a halt at some kind of crossroads. The modern Frankensteins of tyranny, greed, violence, and inhumanity, which in our great cities loom so large, are threats to our very survival and we seem to have lost all reverence for life and for each other.
We will survive as a great and inventive people if we can find a way of life where machines and the money behind the machines cease to be our masters but take their place as a means of enhancing human health and human dignity.
The new epidemics of degenerative disease are not inevitable, nor is their cause mysterious. They are nature's language, telling eloquently of our failure to understand the supreme importance of nature's laws.
Then an old man remarked "It's a marvel to me
That people give far more attention
To repairing results than to stopping the cause
When they'd much better aim at prevention;
Let us stop at its source all this mischief," cried he.
"Come neighbours and friends let us rally;
If the cliff we will fence, we might also dispense
With the ambulance down in the valley.Acknowledgements
Without writing another lecture it is difficult fully to record my thanks to so many helpers.
Professor James Knox and his staff cheerfully and unfailingly gave advice in preparation of slides. Professor Alex Mair put at my disposal his beautifully filed collection of Mackenzie papers. Sir James Mackenzie's niece, Mrs Stewart Thomson, told me willingly about her family and Mr James Reid, late of Picstonhill, told me of the farm. Lady Eve Balfour and Dr Innes Pearse have, over the years, always responded to my queries and arguments; so have Dr Kenneth Heaton, Mr Denis Burkitt, and Professor John Yudkin. Dr Harry Stalker has scouted the medical libraries for references on nutrition on my behalf. Ms Judith Appleby transformed my chaotic sketch into a striking picture.
To them all I would like to record my undying thanks.
I owe a special debt of thanks to Surgeon Captain T L Cleave for teaching me so much, for giving me his time in long hours of argument, and for sharing with me so generously his unique insight into the wonder of nature's processes.
Special thanks also goes to our practice secretary, Mrs Grace McColgan, for typing the script again and again and again!
And how can I sufficiently thank my wife, Sonia, and daughter, Jane, for so valiantly picking and weighing vegetables in snow, sunshine, and storm, and the whole family for tolerating my neglect of other things during this journey with Sir James Mackenzie!References
Ackroyd, W. R. (1967). Sweet Malefactor. London: Heinemann.
Amulree, B. W. S. M. Mackenzie Papers. Department of Social and Occupational Medicine, Ninewells Hospital, Dundee.
Antar, M. A., Ohlson, M. A. and Hodges, R. E. (1964). Changes in retail marketfood supplies in the United States in the last seventy years in relation to the incidence of coronary heart disease, with special reference to dietary carbohydrates and essential fatty acids. American Journal of Clinical Nutrition, 14, 169-178.
Balfour, E. B. (1943). The Living Soil. London (Faber and Faber). Universe Books N.Y. 1975.
British Medical Journal (1971). The Masai's cholesterol. Editorial, 3, 262-263.
Burkitt, D. P. (1971). The aetiology of appendicitis. British Journal of Surgery, 58, 695-699.
Burkitt, D. P. (1973). Some diseases characteristic of modern western civilisation. British Medical Journal, 1, 274-278.
Clayton, M. ( 1978). The Times, 18 April.
Cleave, T. L. 1941). Natural bran in the treatment of constipation. British Medical Journal, 1, 461.
Cleave, T. L. 1956). The neglect of natural principles in current medical practice. Journal of the Royal Naval Medical Service, 42, No. 2, 55.
Cleave, T. L. ( 1960). On the Causation of Varicose Veins. Bristol: John Wright.
Cleave, T. L. (1962). Peptic Ulcer. Bristol: John Wright.
Cleave, T. L. (1974). The Saccharine Disease. Bristol: John Wright.
Cleave, T. L., Campbell, G. D. and Painter, N. S. (1969). Diabetes, Coronary Thrombosis and the Saccharine Disease. Bristol: John Wright.
Connor, W. E. and Connor, S. L, (1972). The key role of nutritional factors in the prevention of coronary heart disease. Preventive Medicine, 1, 49-83.
Craig, J. 0., Ford, J. A. and McCulsh, A. C. (1977). Rising incidence of childhood diabetes. British Medical Journal, 1, 639.
Department of Health and Social Security (1977). Prevention and Health. London: HMSO.
Hall, R. H. (1977). Are the multitudes of fabricated foods really a health hazard protected by law? Science Forum, 10, No. 6, University of Toronto Press.
Hall, R. H. (1978). Is modern food ecologically sound? International Journal of Environmental Studies, 12, 12-25.
Heaton, K. W. (197-1). Bile Salts in Health and Disease. Edinburgh: Churchill Livingstone.
Heaton, K. W. (1973). Foodfibre as an obstacle to energy intake. Lancet, 2, 1418-1421.
Henderson, J. M. (1964). Looking back to Mackenzie. James Mackenzie Lecture 1963. Journal of the College of General Practitioners, 7, 9-23.
Hodges, R. D. (1978). The case for biological agriculture. International Institute of Biological Husbandry. No. 1. Stowmarket.
Hyams, E. (1976). Soil and Civilisation. London: John Murray
Illingworth, C. F. W. (1953). Peptic Ulcer. Edinburgh: E. & S. Livingstone
Jackson, M. (1956). My life at Key River. Journal of Medical Women's Federation, 38, 40-56
Jukes, T. H. (1977). Current concepts in nutrition: food additives. New England Journal of Medicine, 297, 427-430
Kaunitz, H. (1978). Cholesterol and repair process in atherosclerosis, USA. Lipids, 13,373-374.
Kemp, I. W. and Ruthven, M. E. (1978). Cancer in Scotland. Health Bulletin, 36, 105-109.
Lancet (1977). Nitrate and human cancer. Editorial, 2, 281-282.
McCance, R. A. and Widdowson, E. M. (1956). Breads, White and Brown. London: Pitman.
McCarrison, R. ( 1906). The three-day fever of Chitral, and its contribution to the study of the unclassed fevers in India. Indian Medical Gazette, 41, 7-14.
McCarrison, R. ( 1908). A critical analysis of the aetiology, and symptomatology of the three-day fever of Chitral, and an analogy between this condition and Dengue Fever. Indian Medical Gazette. 43, 5-12.
McCarrison, R. (1917). The Thyroid Gland in Health and Disease. London: Balliere & Co.
McCarrison, R. (1921). Studies in Deficiency Disease. London: Oxford Medical Publications.
McCarrison, R. ( 1926). The effect of manurial conditions on the nutritive and vitamin values of millet and wheat. Indian Journal of Medical Research. 14, 351-378.
McCarrison, R. (1936). Aspects of thyroid disease. British Medical Journal, 1, 653.
McCarrison, R. (1953). Nutrition and Health. London (Faber and Faber). McCarrison Society 1982.
McKenzie, J. Papers. Edinburgh University Library.
McKenzie, J. (1919). The Future of Medicine. London: Frowde, Hodder & Stoughton.
Mackenzie, J. (1926). The Basis of Vital Activity. London: Faber & Gwyer.
McKeown, T. (1976). The Modern Rise of Population. London: Edward Arnold.
McMichael, 1 (1977). Diet and coronary heart disease. British medical Journal, 1, 1467-1468.
Mair, A. (1973). Sir James Mackenzie, MD, 1853-1925, General Practitioner, Edinburgh & London: Churchill Livingstone.
Malines, J. (1953). The fence or the ambulance. Journal of the Soil Association, 7, No. 4, 24.
Mann, G. V., Shaffer, R. D., Anderson, R. S. et al.(1904). Cardiovascular disease in the Masai. Journal of Atherosclerosis Research, 4, 289-312.
Medical Research Council Working Party Report (1970). Dietary sugar intake in men with myocardial infarction. Lancet, 2, 1265- 1271.
Michaels, L. (1966). Aetiology of coronary artery disease: an historical approach. British Heart Journal, 28, 258-264.
Milton, R. F. (1975) in The Living Soil and The Haughley Experiment. Ed. Balfour, E.B. London: Faber.
Office of Health Economics (1975). Information Sheet 26. London: OHE.
Painter, N. S. and Burkitt, D.P. (1971 ). Diverticular disease of the colon -- a deficiency disease of Western civilisation. British Medical Journal, 2, 450-454.
Price, W. A. (1939) Nutrition and Physical Degeneration, Price Pottenger Foundation, La Mesa, California.
Rowlands, M. J. and Wilkinson, B. (1930). The vitamin B content of the grass seeds in relationship to manures. Biochemical Journal, 24, 1.
Schaefer, 0. (1959). Medical observations and problems in the Canadian Arctic. Canadian Medical Association Journal, 81, 386-393.
Schuphan, W. (1974). Nutritional value of crops as influenced by organic and inorganic fertilizer treatments. Qualitas Plantarum, 23, No. 4, 333-358.
Scottish Home and Health Department (1977). Health Services in Scotland. Edinburgh: HMSO.
Stefansson, V. (1960). Cancer: Disease of Civilisation? New York: Hill & Wang.
Thornson, J. (1975). Should modern food carry a government health warning? World Medicine, 10, No. 25, 74-81.
Todd, J. E. and Whitworth A. (1974). Adult health in Scotland, 1972. London: HMSO.
Trenchard, Lord. (1977). Fat consumption -- long term trends. Health and Hygiene, 1, No. 2, 77-82.
Ward, B. (1976). The Home of Man. London: Deutsch.
Wilson, R. McN. (1926). The Beloved Physician. London: John Murray.
Wood, P. H. N. ( 1971). Rheumatic complaints. British Medical Bulletin, 2-7, 82-88.
Wrench, G. T. (1938). The Wheel of Health. C W Daniel.
Wylie, J. C. (1959). The Wastes of Civilisation. London: Faber.
Yudkin, J. (1972). Pure, White and Deadly. London: Viking.
See also:
Article on butter by Weston A. Price, "Are the Activators Revealing The Nature of Life in Health and Disease Including Dental Disease?", Cleveland, Ohio 1932:
http://www.westonaprice.org/Weston_archive.htm
"The Case for Butter" by Trauger Groh:
http://www.price-pottenger.org/Articles/Case_for_butter.html
Medical Testament
The Nature of Health (Introduction and Table of Contents)
Medical Testament
References
McCarrison bibliography (References)
Speeches by Sir Robert McCarrison and Sir Albert Howard
Correspondence in the British Medical Journal
Food and Health -- Lionel Picton
Soil Fertility and Health -- Sir Albert Howard
Soil Fertility: The Farm's Capital -- Sir Bernard Greenwell
Open-Air Dairying -- A.J. Hosier
Farming for Profit with Organic Manures -- Friend Sykes
Nutrition and Health -- Sir Robert McCarrison
Nutrition in Health and Disease -- Sir Robert McCarrison
Studies in Deficiency Disease (Introduction) -- Sir Robert McCarrison
Diseases of Faulty Nutrition -- Sir Robert McCarrison
Nutrition and Physical Degeneration -- Weston A. Price
The Saccharine Disease -- T. L. Cleave
An Agricultural Testament -- Sir Albert Howard
Ill Fares the Land -- Dr. Walter Yellowlees
Food & Health in the Scottish Highlands: Four Lectures from a Rural Practice -- Dr Walter Yellowlees
Back to the Small Farms Library Index
Community development | Rural development
City farms | Organic gardening | Composting | Small farms | Biofuel | Solar box cookers
Trees, soil and water | Seeds of the world | Appropriate technology | Project vehicles
Home | What people are saying about us | About Handmade Projects
Projects | Internet | Schools projects | Sitemap | Site Search | Donations | Contact us