|
 |
Part 2
Food & Health in the Scottish Highlands
-- Four Lectures from a Rural Practice
|
|
Introduction
1. Land Use and Nutrition in a Highland Valley
2. Why "Wholefood"?
3. The Chain of Health: Soil Fertility and Food Quality
4. An Ecological Approach to Modern Diseases
See also:
Ill Fares the Land -- Dr. Walter Yellowlees
3. The Chain of Health: Soil Fertility and Food Quality
The study of the relationship between soil fertility and human health has always been of the utmost interest to the Soil Association. One of our most distinguished members, the late Professor Lindsay Robb, a man of wide experience as a practical farmer, teacher and administrator, repeatedly advocated that such was the dependence of human health on agriculture, that the Ministries of Agriculture and Health should be combined in a single Ministry of Land Use. (1)
What evidence have we of this dependence of health on agriculture, or of superior quality in organically grown crops? Experimental evidence to satisfy the laboratory purist will always be beyond our reach. The conditions of control and duration in any feeding trial designed to discover an effect on human health of organic versus chemically grown food must for ever be too severe and impracticable to be tolerated in a free society. We can only look at the evidence which so far has been recorded and published; and those of us engaged daily in the tasks of growing crops and rearing animals must be guided by our own experience. We would do well to remember that in biological research results obtained by even the most sophisticated scientific experiments have to be tempered by common sense -- particularly those experiments financed by someone who has something to sell.
One truth is fundamental in our understanding of the human predicament; it was stated by Sir Robert MacCarrison after a lifetime of medical research. (2) It is as follows: "Of all factors which make human health, the greatest single factor is adequate food". (Sir Robert used the phrase "perfectly constituted food".) The converse is also true, that the greatest single factor in causing disease is inadequate food.
Agriculture provides the raw materials for the bulk of our food; surely it must follow that the quality of those raw materials has a vital bearing on human health. Even if we do not yet know with precision exactly how the quality of food is enhanced or reduced by different methods of soil treatment, we do know quite a lot about man's manipulation of the earth's green crust for his own nourishment.
For a period of some ten thousand years of settled agriculture, man has freed himself from an existence of hunting and gathering. In the civilisation which without settled agriculture is impossible he has taken edible seeds and plants, and he has improved these and prepared them for human and animal consumption; he has manipulated nature in two main areas of food production. The first area is between seed bed and harvest -- his preparation of and treatment of the soil. The second is between harvest and dinner plate. In Figure 1 I have tried to make a picture of the two areas of manipulation, and the grasping, hungry hands of man.
Manipulation of the seed bed includes what those hands do to forest as well as prairie.
Let us look at the first area.
We humans, unlike the animals who seek their food, driven by blind instinct, are burdened by consciousness, by choice, and by our own conflicting emotions. In our manipulation of nature (as in many other transactions) emotions charged with arrogance and with avarice have, alas, throughout history been all too dominant.
When blind ignorance is added to arrogance and avarice the results on the soil have been devastating.
The eroded soils and deserts of the Mediterranean seaboard. the dust bowls and deserts of North America and Africa, the desolate ruins of the great Babylonian and Assyrian empires are all the result of extractive farming, of growing for today's yield rather than for tomorrow's fertility.
In their book "The Rape of the Earth" (3) Jacks and Whyte wrote: "Men are permitted to dominate nature on precisely the same conditions as trees and plants, namely on condition that they improve the soil and leave it a little better for posterity than they found it." Please note that nature has her conditions; her society is not a permissive one. If we ignore her conditions she hits back.
On the eroded soils of these continents, nature writes the story of her revenge: thanks to modern machines and modern chemicals, the destruction of the soil in the present century has exceeded in speed and in scale anything which went before. Jacks and Whyte calculate that more soil was lost from the world between 1914 and 1934 than in the whole of the previous human history.
In the wake of this awful spoliation whole civilisations have lost their vigour and perished. Is it then only the absurd and fanciful dreams of a few cranks to suggest that Northern Europe where a high rainfall, temperate climate and traditional mixed farming have so far maintained the integrity of the soil, we abandon our traditional methods at our peril?
Whatever chemicals do to the soil and to our health they certainly do not leave our surface waterways better than before, or improved for posterity. In some areas so much nitrate has run off the fields into water supplies that warnings have recently been given on the dangers to infants of nitrate poisoning, if untreated drinking water is used for making up baby foods.
So we can define two different approaches to the first area of manipulation -- organic and extractive.
Organic does not simply mean using dung rather than chemicals: it means so treating the soil as to enhance its fertility for the future in the belief that if this is your aim, your crops, and the creatures that feed on them will be healthy and so will your environment.
Chemical or extractive farming means growing for today's highest yield and never mind tomorrow's fertility.
The conflict between the two is well seen in a scrap of conversation I had with one of my farmer patients many years ago. We were discussing his potato crop. "Well doctor", said this farmer, "I use plenty of yon compound fertiliser for the tatties I grow for cash. But for the tatties we eat ourselves --- I just gie them plenty o' dung."
If you were to ask me what human diseases this farmer would be preventing by using dung rather than chemicals I would have to reply that I could name none.
But I would hasten to add that just because a quality of food cannot yet be measured it does not follow that such quality is not there.
I would refer you to the writings of Sir Albert Howard, one of the founders of the organic movement. Howard's views on health and disease in agriculture (4) may be challenged by those scientists who will believe nothing unless it can be proved by meticulously controlled studies under laboratory conditions. But you slmply cannot put a whole farm and the community that feeds from it in a laboratory. It was dissatisfaction with the fragmentation of knowledge by laboratory-bound research which compelled Howard when he went to India in 1905 as Economic Botanist at the Agricultural Research Institute at Pusa, Bengal, to try a completely new approach to the problem of eradicating disease from crops. He studied the methods of the peasant farmers of Pusa who without any modern aids, year after year seemed to maintain the fertility of their soils and the health of their crops. Howard copied and perfected composting methods used by those peasants and elsewhere in the East.
"By 1910" he wrote, "I had learned to grow healthy crops, practically free from disease without the slightest help from mycologists, entomologists, bacteriologists, agricultural chemists, statisticians, clearing houses of information, artificial manures, spraying machinery, insecticides, fungicides, germicides and all other expensive paraphernalia of the modern experimental station. This preliminary exploration of the ground suggested that the birthright of every crop is health".
Howard showed that the farm animals nourished on organically grown crops resisted disease. He gave examples of human groups, schools and other communities, whose resistance to infection and general health seemed greatly improved when their food was organically grown.
These observations among human groups would not satisfy the criteria for a scientific experiment. There were no control groups, but nonetheless they gave strong support to Howard's belief that the health of soil, plant, animal and man formed one continuous chain. Even stronger support came from the work of Sir Robert McCarrison.
McCarrison worked from the human end of chain; his approach to the problem of health and disease was remarkably similar to that of Howard. In the Indian Medical Service he was surgeon to the Gilgit Agency in the Northern Frontier of India from 1904 to 1911. There he found a people whose health, vigour and longevity were an astonishing contrast to the disease ridden populations of civilisation and to the stunted, unhealthy people of many of the Southern Regions of India.
During the seven years of his work among these Northern people he saw not a single case of stomach ulcer, appendicitis or cancer.
He noted that the Hunzas and Sikhs were superb farmers and gardeners wholly dependent on their own produce which they grew by careful methods of composting. They returned all their wastes to the soil; their cereal was unrefined whole wheat, and they ate no sugar.
McCarrison realised that here was a phenomenon worth studying -- health. He later carried out many feeding experiments on animals which confirmed his belief that the health of these human groups was due primarily to their nutrition.
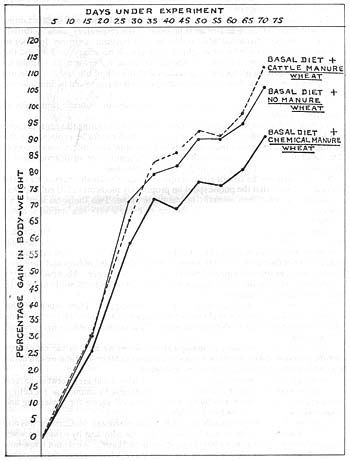
In one of his experiments (5) the growth rate of rats was shown to be reduced (by 10%-17%) when their ration of wheat was grown on soil fertilised by a complete chemical fertiliser, rather than cattle manure. The cattle manure wheat gave consistently better results as judged by growth rate and seemed to have a far higher vitamin A content than the chemical wheat. (Fig. 2).
Fig. 2. -- Chart showing the order of nutritive value of the three wheats: 'cattle manure wheat' has the highest value; 'no manure wheat' the next highest; and 'chemical manure' wheat' the lowest value.
In this same experiment organically grown millet was shown to have a higher vitamin B content than chemically grown millet, and to have a much higher protein content.
In these experiments with millet and wheat, organic methods thus seemed to give nutritive values measurably superior to chemical methods, but in the case of millet the yield by chemical methods was greater.
In the journal "Qualitas Plantarium" Werner Schuphan in Germany has published an interesting account of a twelve year experiment in which a variety of, vegetable crops were grown on plots fertilised in four different ways: N.P.K. alone (Nitrogen, Phosphate, Kalium (Potash)), stable manure plus N.P.K., stable manure alone and biodynamic compost. The organic fertilisers on average gave a much lower yield than the chemical but the dry matter, protein, vitamin C, total sugars and minerals were higher in the organically grown crops. The latter included spinach, lettuce, savoy, potatoes, celeriac, carrots, fodder and sugar-beets.
A similar difference in quality of organically grown crops was demonstrated at the experimental farm at Haughley in Suffolk, set up just before the last war thanks to the vision and dedication of the late Miss Alice Debenham and Lady Eve Balfour, and later taken over by the Soil Association.
Cows fed on organically grown fodder consistently gave more milk from less food than cows fed on pastures whose growth was boosted with soluble chemicals. (7) As in the case of the other experiment, the organically grown produce seemed to have some quality which the other lacked. The story of the Haughley Experiment will be told next year when Lady Eve Balfour is to publish a new edition of her book "The Living Soil". (22)
These three experiments, carried out in completely differing times and places, seem to show a definite superiority in the quality of organic crops, even though in some cases, yields were lower. Perhaps my searching has lacked diligence -- but there seems to be a remarkable absence of any other serious study of this vital subject, the relationship of food quality and health to soil fertility. Hence the enormous importance of the reports of scientists like McCarrison who have been able to participate in nature's own experiments by observing the health and physique of peoples isolated from industrial man's foods.
From the observations made in many parts of the world (8) (9) (10) (11) (12) (13) (14) it is abundantly clear that people who have no access to Western man's foods and who have a reasonably varied and plentiful food supply, have a remarkable immunity to the degenerative diseases which are so widespread in Britain today, and a high resistance to the effects of many infections.
The diseases of mankind are in two main groups, infection and degeneration. The commonest infection in Britain is invasion of the respiratory tracts -- throat, ears, nose, sinuses, bronchial tubes and lungs -- by bacteria or viruses. In order to combat this invasion a colossal weight of antibiotics is necessary. In England the annual number of prescriptions for antibiotics alone is between 33-34 million. Without this artificial protection it is certain that the toll of life and the suffering from pneumonia, bronchitis and suppurating ear infections would be much worse than it is.
So we are protected for the time being by this antibiotic umbrella from some of the effects of infection.
We have no comparable protection from degeneration: during this century there has been a massive rise in degenerative diseases which cannot be explained by the ageing population; many of these diseases like duodenal ulcer affect young people. The amount of suffering and disability from the rising tide of degeneration is beyond calculation. The cost to the Nation is tremendous.
In 1972 in Britain the cost of all prescriptions under the Health Service was 319 million pounds sterling; on top of that the public spent on proprietary medicines 120 million pounds; that is a total of 439 million pounds annually on medicine alone. Two thousand tons (15) of aspirin are swallowed every year in Britain. We are a very sick nation and our sickness is not getting better.
Some years ago in the Annual Report of the Department of Health for Scotland (16) we read "In terms of hospital attendance and demands for hospital treatment it might seem that ill health is increasing. There is no simple satisfactory explanation of the fact that better disease control, the saving of lives and improved environment are still accompanied by heavy sickness incidence". I believe there is a satisfactory explanation; it is, I repeat, that the greatest single factor in keeping us healthy is adequate nutrition.
Our nutrition in Britain today is totally inadequate. How much of this inadequacy is due to extractive chemical farming, we do not know. But surely we do know enough to cry halt to the present policy of ever more chemicals in every part of the world.
So much for the first area of manipulation. When we look at the other area between harvest and dinner plate we are on much sounder ground and we can detail the inadequacy of Britain's food with confidence.
My sketch (Fig. 3) shows four main ways in which food is altered between harvest and dinner plate. Firstly, by robbing it of its freshness by canning or packeting, secondly by over-cooking, thirdly by adding chemical agents for preserving and colouring, fourthly by carbohydrate refining.
Green leaf foods are profoundly altered by minimal storage: McCarrison was one of the first workers to show that Vitamin C was speedily lost by oxidation when vegetables were allowed to lie between gathering and eating. We do not know how much Vitamin C we need for health but some surveys have repeatedly suggested that among the elderly and even among some university students the intake of this unique vitamin is well below the recommended level. (21)
We do not know what vital food factors other than certain vitamins are lost when perishable foods are stored or canned, so fresh vegetables often eaten raw are an essential part of agricultural man's food. Without them his resistance to disease is lowered.
The implications for agriculture for the future are clear. Production of home-grown foods must be enormously expanded. We must close the awful gap which in urban societies has widened between the population and its perishable vegetables and fruits. There is, I believe, no other way of ensuring an adequate intake of vitamins and other fresh food factors vet to be discovered. This means expansion of market garden areas in and around our towns. It means, I believe. completely rethinking the structure of society with its over concentration of population in huge urban areas.
The fourth way in which food is altered. carbohydrate refining, is so important that I make no apology for repeating what has already been said on this subject in an earlier edition of this journal. (17) Carbohydrate is our cheapest form of energy-giving food: the energy comes from glucose in the blood. Blood glucose, or blood sugar, is derived from starch in cereals or roots and from sugar in various roots, crops and fruits. Our bodies were evolved to get their sugar from these natural sources.
From days of antiquity some peoples -- usually the richer classes -- sifted their wheat flour to make it whiter; but, thanks to his machinery, in the last 170 years modern man has released highly refined white flour to the mass of populations for whom it is now the staple carbohydrate. Whole wheat bread is used by a tiny minority.
Again thanks to his machines and technology modern man has extracted pure sugar from cane or root and one of the most astonishing changes in food habits in the last 160 years has been the staggering rise in consumption of sugar, from around about 12 pounds per head per annum in 1815 to about 120 pounds per head per annum today.
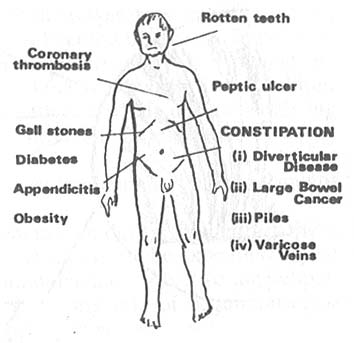
Fig. 4. -- The effects of Carbo-hydrathen refining on human health (T. L. Cleave).
Our bodies were not built to cope with highly refined flour or with pure sugar. The research worker who more than any other has elucidated the effects of refined carbohydrate food is Captain T. L. Cleave. His book "The Saccharine Disease" (18) is essential reading to all thoughtful people.
The effect on our bodies of this onslaught of refined carbohydrate is devastating; I have tried to show in Fig. 4 the essence of Cleave's hypotheses. The epidemiological evidence collected by Cleave shows a constant relationship between the occurrence of these diseases and the consumption of refined carbohydrate.
Perhaps a better way of demonstrating the extent of degenerative disease from this cause is to show you a corner of my practice. Fig. 5 is a view of the valley where I live and work.
If we were to take a bird's eye view of the valley from where the sketch was made and took down on the farms and cottages spread out along about a mile of river, and if we were to map out some of the diseases endured by the people living there, the result would be as in Fig. 6. These patients are all countrymen and women doing hard physical work. Lack of exercise could not have contributed to the cause of their diseases. In the seven cases are three farmers, two gamekeepers and two housewives; all had their illness at comparatively young ages. Two of the farmers died (one aged 52), the third had to retire prematurely, and one of the gamekeepers also had to retire aged 60. All cases except one had upper and lower dentures. None of the men were cigarette smokers.
If diseases like coronary heart disease and duodenal ulcer were due to stress, to the rush and din of modern city life, they would be extremely rare in the tranquillitv of our practice area. But they are not; the little bit of the practice which I have described is not unique. This pattern of disease is seen all over the Highlands.
Fig. 7 illustrates the tragedy of rural Scotland. The mill which once ground locally-grown oats and barley is a mouldering ruin. The land which used to be the source of nourishment is underused, neglected. Nourishment now comes from that van, its shelves crammed with tins of all description, with sliced white loaves, highly coloured and sweetened cakes and biscuits and soft drinks.
So my patients suffer vitamin deprivation and also lack of elements in fresh food, which I am sure exist but which are yet to be discovered. They stuff themselves with white flour and sugar products. So their teeth, arteries and bowels rot, their digestions are impaired, their hormone systems unbalanced. (20) On their stricken bodies nature writes the story of her revenge -- revenge for manipulating food between harvest and dinner plate NOT in the interests of health but trade.
The implications for the future are clear. An awakened public must demand from its farmers and food industry food which is fresh, whole and grown on fertile soil; if to do this the basis of our economic life has to be altered -- we simply must change.
There is, in any case, abundant evidence that our present economic system with its over-industrialisation has failed. No longer can we depend on the output of our industries to buy food from abroad; concentration on industrial expansion at the expense of agriculture has completely failed to give health to our bodies, peace to our minds, or satisfaction in our work and human relationships. We are, I repeat, a sick nation; our sickness, like that of earlier civilisations, comes from arrogance and avarice compounded by ignorance; ignorance above all of the fact that you cannot apply to biology the rules and yardsticks of factory-based industry. Biology is the study of life; where there is life there must be reverence. Nature has her strict conditions for the life of soil, plant, animal and man. Only by obeying nature's laws will this country get back on the road to health and sanity. There is no other way; the broken chain must be mended.References
1. Robb, Prof. Lindsay, Sanderson-Wells Lecture 1975, J. Soil Association. 17.2.1972.
2. McCarrison, Sir R., Nutrition and Health. Faber 1961.
3. Jacks, G. V., Whyte, R. 0., The Rape of the Earth. Faber 1949.
4. Howard, Sir Albert, Farming and Gardening in Health and Disease. Faber 1945. An Agricultural Testament. Oxford University Press. 1940.
5. McCarrison, Sir R. , Ind. J. Med. Research, Vol XIV. 1926.
6. Schuphan, W., Qual. Plant. Pl. Fds. hum. nutr. XXIII, 4:333-358. 1974.
7. The Haughley Experiment. Annual Report 1964, p.37. Soil Association , New Bells, Haughley.
8. Price, Weston, A., Nutrition and Physical Degeneration, 1939 Los Angeles. Published by author.
9. Schaeffer, Otto. Canad. M.A.J. Sept. 1, 1959. 87. Medical Observation and Problems Canadian Arctic.
10. Stefansson, V., Cancer. Disease of Civilisation? Hill & Wang, New York. 1960.
12. Burkitt, D., World Medicine. Feb. 1971. Diet and Disease.
13. Aravantis, Prof. C., Cardiology Today. Vol. 2, No. 2. 1974. Excerpta Med. Found. "The Classic Way of Life."
14. Burns-Cox, C. J., Cardiology Today. Vol. 2, No. 4, 1974. "The End of Splendid Isolation."
15. B.M.J. 1974, Vol. 3. 5. Leading Article. "Aspirin and What Else."
16. Annual Report Dept. of Health for Scotland, 1954. p. 15. H.M.S.O.
17. Yellowlees, W. W., Jour. Soil Association. April 1963.
18. Cleave, T. C., The Saccharine Disease. John Wright & Sons, Bristol. 1974.
19. Yellowlees, W., Update. 1972. Vol. 4. 12. Stress and Disease.
20. Ziegler, E., Zeitschrift fur Kinderheilkunde. 99. 146-166. 1967. Secular changes in the stature of adults and the secular trend of modern sugar consumption.
21. Howard, A. N. and McLean Baird. Nutritional deficiencies in modern societies. Food Education Society. 1973. Newman Books Ltd.
22. Balfour, Lady Eve. The Living Soil. Faber.
4. An Ecological Approach to Modern Diseases
I had never heard of the word 'ecology' until after I had qualified in medicine in 1941. During my undergraduate years, it was never suggested to students of medicine that, without an understanding of ecology, many of the diseases encountered daily in our hospitals could only be seen as meaningless, haphazard strokes of fate. Take, for example, the teaching on a common disease, acute appendicitis. Emphasis was put on diagnosis, differential diagnosis and pathology. In the surgical wards of large teaching hospitals the regular admission of cases of appendicitis gave plenty of opportunity for students to learn about the techniques of a usually simple operation. Indeed, for the budding young surgeon, cases were welcomed. All this is understandable. A doctor who cannot confidently diagnose a common abdominal emergency or a surgeon unable efficiently to operate are a danger, and should be failed in their examinations.
But none of my teachers told me of the following two features of appendicitis which are as important as the intricacies of diagnosis and treatment. Indeed in some ways they are more important because they suggest a simple cause and so, the means of prevention.
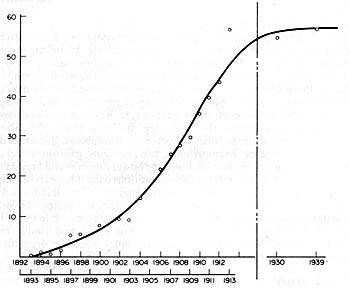
Fig. 1. Operations for appendicitis at the Edinburgh Royal Infirmary. Appendicectomies are shown per 1000 total admissions between 1892 and 1913. Figures for the years 1899, 1901 and 1905 are not available. (From the Edinburgh Hospital Reports, Archives Department, Royal Infirmary, Edinburgh).
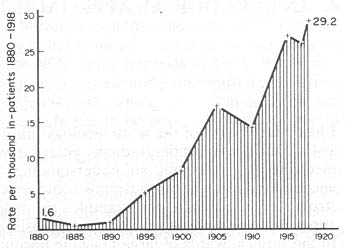
Fig. 2. Cases of acute appendicitis at the Bristol Royal Infirmary. (From A.R. Short, Br. J. Surg., 8, 171, 1920.)
Firstly, until the closing decades of the 19th century appendicitis was a rare condition -- almost unknown, but it increased rapidly during the first three decades of the 20th century (Figs. 1 and 2). Secondly, among isolated people, living beyond the trade routes of industrial societies, appendicitis does not occur. (1).Diseases of Civilisation
The significance of these two features of the epidemiology of one disease is greatly enhanced by the knowledge that they are shared by many other non-infective (or degenerative) diseases which, because of their association with an industrial way of life, can accurately be classed as 'diseases of civilisation'.
Four characteristics of diseases of civilisation are of great interest to the ecologists.
- They are rare or unknown among 'primitives';
- Primitives of any ethnic group get these diseases when they emigrate to or are engulfed by 'civilisation';
- They tend to appear together, often in the same patient;
- They have increased greatly in the last hundred years or so.
The word 'primitive' is used to describe those communities whose isolation makes them totally dependent on their own resources and unsophisticated technologies for their daily living. As the trade routes of the world penetrate ever further, such people are fast disappearing.
Along with appendicitis the following diseases share the above four characteristics; dental decay, obesity, coronary thrombosis, diabetes, duodenal ulcer, diverticular disease, haemorrhoids, varicose veins, gallstones, and probably certain common forms of cancer such as large bowel cancer (2) and breast cancer (3).
In their thousands sufferers from these conditions daily throng consulting rooms, clinics and hospitals throughout the United Kingdom and in all industrial nations. Coping with them requires a vast expenditure of money and manpower. Since many of these degenerations are slowly progressive they are responsible for an immense amount of disability. Clearly if we knew their cause and could remove it, improvement in the health of all industrial peoples would be dramatic and the saving in money and manpower incalculable.Mind and Body
If only we could identify those harmful environmental changes which take place when human beings progress (if it is progress) from primitive to civilised. No experiment could possibly be devised which would so control and manipulate a human sample for a sufficient time to identify and to assess the multitude of variables.
For a time, after the last war, it became fashionable to blame emotional and psychological factors. An enthusiastic school of psychosomatic medicine found in psychoanalytic theory an explanation for duodenal ulcer, coronary thrombosis, hypertension or even diabetes (4). Others placed more emphasis on 'stress', particularly the stress of the city with its hurry, crowds, impersonal tower blocks and traffic jams (5).
In reviewing those psychological factors, experience of general practitioners in areas such as the Scottish Highlands is of great importance. Here, life in the villages, although changed by the coming of the motor car and the tractor, has in many ways continued at the slow tempo of former years. There is no rush and little thrusting for status; a sense of community is strong and family life possibly more stable than in the cities.
Yet all the diseases mentioned above appear to be as common in the Highlands as elsewhere. Duodenal ulcer, coronary thrombosis and hypertension are frequent causes of death and disability from which farmers, gamekeepers and foresters enjoy no immunity.Disease Clustering
The clustering of various diseases of civilisation in one individual is a remarkable phenomenon which receives little comment. Here are three examples:
Mr. A, schoolmaster, born 1916, edentulous and wore upper and lower dentures, duodenal ulcer diagnosed 1962, diverticular disease diagnosed 1970; coronary heart disease diagnosed 1975, died from coronarv thrombosis in 1978.
Mr. B, gamekeeper, born 1913; edentulous; duodenal ulcer diagnoscd 1969; coronary heart disease diagnosed 1970; suffered a stroke 1974.
Mr. C, gamekeeper, born 1915; edentulous, diverticular disease diagnosed 1970; diabetes diagnosed 1970; coronary heart disease diagnosed 1977, died from coronary thrombosis 1982.
Such clustering is so common in medical practice that it seems to be accepted without thought. Possibly one reason for this neglect is the ever increasing specialisation in medicine. Most diseases are now subjected to intense study in specialised departments, where little thought is given to other major diseases from which the patient under study may have suffered. Registrars eager to get their names into print take one totally obscure fragment of a biological process and subject it to the closest scrutiny without giving thought to the broad setting of which that particular process is a very small part. Surely the repeated appearance of diseases associated one with another in the same patient argues a common cause.
What then happened to the three men referred to above and to the millions of men and women like them? They have no teeth, they are quite unable to maintain the integrity of their gut, their cardiovascular and endocrine systems.
From my long experience of families and their illnesses I believe that psychological factors can be ruled out as important causes; sometimes emotional stress can trigger off a heart attack or an acute episode of one disease or another, but I believe that we must seek elsewhere for the underlying cause.Food and Health
Medical opinion increasingly tends to accept that the food of industrial people is the most likely cause for the diseases of civilisation. But here again we encounter the sad fact of disagreement among scientists. If faulty food is the cause there is no agreement at all on what is the main fault.
An excess of animal or saturated fat currently enjoys prominence as the main cause of our downfall, particularly as the cause of coronary heart disease, but evidence supporting this theory is not at all impressive (6, 7).
The difficulty of finding our way through a fog of conflicting theories is made no easier by the part played by commercial interests enjoying all the power which stems from huge expenditure on advertising. A law which would compel every contributor to the medical and lay press on the subject of nutrition and health to reveal whether or not he or she is receiving a salary from any branch of the food industry would help the reader to judge the true value of such contributions.McCarrison, Cleave and Burkitt
To the ecologist the writings of three men stand as beacons throwing light on the diseases of modern man and on their causes. They are the late R. McCarrison (8), T. L. Cleave (2) and D. P. Burkitt (9). All three present the same hypothesis which, broadly, is as follows.
Man is perfectly adapted to his food supply as it occurs in nature. He is omniverous and if he eats a varied diet of natural food, his growth, stature and health will be sound and compatible with normal lifespan. The greatest single cause of disease and death is malnutrition; the inability of a large proportion of the world's population to secure an adequate intake of food is the main cause of diseases of poverty such as tuberculosis, anaemia, gastro-enteritis and kwashiorkor. Death rates from pneumonia, dysentery, whooping cough and even malaria are invariably higher in malnourished populations.
In advanced countries death rates from infections and from diseases of poverty have been greatly reduced but they have been replaced by the diseases of plenty, some of which I have enumerated above. Here the cause is not an inadequate intake of food but the sophistication of food by complex industrial processing. In 1920-1930 McCarrison showed how multiple deficiencies due either to poverty or industrial sophistication lowered resistance to infection and to many forms of degeneration. Since the Second World War Cleave has elaborated the ill effects of carbohydrate refining, his lead was enthusiastically followed by Burkitt who concentrated on diseases caused by fibre deficiency. The most harmful manipulations of food of industrial people are listed below.
Over-cooking and preserving
Convenience foods, the consumption of which has increased greatly over the last few decades, are pre-cooked and require only re-heating for their preparation. The over-cooking to which they are subjected deprives them of heat-susceptible vitamins and fresh food factors of which we may yet be ignorant. We know that ascorbic acid is rapidly lost from green leaf vegetables after they are cut and gathered but what other fresh food factors are also lost?
Carbohydrate refining
Varying fractions of fibre, minerals, vitamins, proteins and oil are all discarded in the refining of wheat flour, and in the extraction of sugar from cane or beet. Of all the processes to which food is subjected in industrial countries, possibly the refining of carbohydrate has the most devastating and widespread effect on human tissue. This will be discussed below.
Food additives
The use of artificial colouring agents, preservatives, synthetic flavouring agents and emulsifiers has greatly increased since the Second World War. One estimate of the consumption of additives in the United Kingdom gives the astonishing figure of 3.2 lb per head per annum
Agricultural residues
The present-day farmer seems compelled to use an ever-increasing tonnage of highly toxic pesticides to protect his crops. Synthetic hormones are also used extensively to promote growth in cattle, as are antibiotics for treatment or for prevention of various diseases. Toxic chemicals are now used to preserve crops such as wheat or potatoes in storage as well as in the fields (11). The long-term effects on human tissues of additives and agricultural residues are quite unknown. Statutory feeding tests with animals will never fully predict consequences of long-term ingestion by human beings of even small doses of man-made chemicals.
The drugs Thalidomide and Practolol had to be hastily withdrawn after untold misery had been caused by their unpredicted side effects. Both had been fully tested. To consumers, concerned about the possible harmful effect of food additives, the law on labelling seems to be remarkably lax. For instance, the Department of Agriculture has refused to compel manufacturers to show on labels whether or not their products contain a widely used dye, tartrazine, a substance which is known to cause distressing symptoms in susceptible individuals (12). These include flushing, blurred vision, and skin rashes. This dye is widely used in some brands of breakfast cereals, biscuits, confectionery, chocolate, ice creams, packaged dessert food mixes, canned vegetables, soup, meat, fish, pickles, snacks and soft drinks. A spokesman for the Food and Drink Industries is quoted (The Times, 14 June 1981) as stating, "In France where they have more detailed labelling, scare stories have stopped people from buying food which contains certain additives. We don't want that to happen here". This statement perfectly focuses the conflict between the needs of trade and the needs of human health. The spokesman quoted above is really saying, "We in the Food and Drink Industry are scared to tell people what we are putting in their food and drink". He is, of course, justified in fearing that well-informed consumers would stop buying products heavily laced with additives. Refusal by the public to buy foods adulterated in this way, and a rising demand for fresh, natural food, if strong enough, might bring about far-reaching changes in the production and marketing of food. This might lead to re-appraisal of land-use and of the balance between agriculture and industry in all advanced countries.Carbohydrate Refining
Fears about the effects of food additives and chemical residues may be unfounded; it is unlikely that scientists will ever be able to know with precision what these potentially harmful chemicals do to human tissues. But thanks to the researches of T. L. Cleave, our knowledge of the ill effects of carbohydrate refining is more complete. The two commonly used refined carbohydrates in Britain are refined flour and sugar. Since the early decades of the 19th century white bread from sifted flour has been eaten by all sections of our population. For all but a very small minority -- about 2% of the population -- it remains the bread of choice.
Sugar with Everything
In the 19th century a rapid increase in the consumption of sugar was the most remarkable change ever to affect the food of mankind. Just why the human craving for the taste of sweetness in food should be so strong remains unknown (13) but the strength of this craving has made profitable the planting of vast acreages throughout the world with sugar cane or sugar beet.
Before the coming of the machine age, refined sugar would have remained an expensive luxury, available only in small quantities to the rich. Without slaves an 18th century farmer, relying on the simple technologies powered by human or animal muscle, could never have produced refined sugar in quantities sufficient to make it an abundant and cheap source of calories. Nor could he have afforded the wasteful use of land which requires 8-10 tons of sugar cane to make one ton of sugar. Only the use of slaves on an unprecedented scale brought an increasing tonnage of sugar to Europe.Sugar and Slavery
In 1510 the first consignment of slaves was shipped from Africa to the Portugese sugar plantations in Brazil and within a decade some 10,000 of them were working there. In their newly acquired possessions in the Caribbean. the Spaniards soon found African slaves far more satisfactory as plantation labourers than the native Arawak Indians. The latter, an unwarlike people, who enjoyed dancing, ball games and pipe tobacco, when subjected to forced labour. simply died in huge numbers.
Slavery, pioneered by the Portugese and Spanish for the expanding sugar trade, was enthusiastically continued by the British and the French. At least 20 million slaves were transported from Africa to the Caribbean and to the American mainland during the centuries of the slave trade and about two thirds of them worked on sugar production (14).
From the 17th century, trade in sugar began to occupy a place in our national economy to be compared with trade in oil today and the wealth created by sugar helped to launch the Industrial Revolution (15).
Thus the spread of sugar cane from the Old to the New World had a profound effect on the European economy; we are still experiencing the political consequences of the forced migration of populations from West Africa to the Americas.
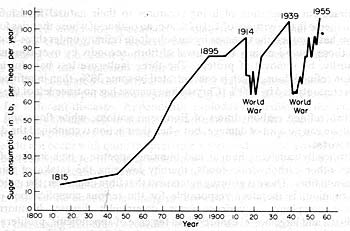
The tax on imported sugar was lifted in 1840 and from then on consumption increased rapidly and steadily to a peak in the 1960s of approximately 120 lb per head per annum (Fig. 3). Yudkin (16) has pointed out that we now eat in two weeks the weight of sugar which 200 years ago took us a whole year to consume.
Fig 3. Sugar consumption in the United Kingdom between 1815 and 1955. (From T.L. Cleave, The Saccharine Disease, p. 7. John Wright, Bristol, 1974.)
Sugar and Health
A hint that the economic and political consequences of the sugar trade would in time be matched by changes in patterns of disease was given by a German visitor to the Court of Queen Elizabeth 1. In 1598 he noticed the blackened, decayed teeth of the virgin Queen and wrote that this was a defect that English seem subJect to from their great use of sugar (17).
Dental caries is one of the earliest manifestations of our rising sugar consumption. In the Middle Ages when refined sugar was rare and very expensive, the level of decay was not much worse in Britain than it had been in Neolithic times (8). But from the 17th century onwards the rise of decay, at first among the wealthier classes, was steady and catastrophic.
In a worldwide survey in the 1930s the American dentist Weston Price (19) found the same pattern of dental disease wherever he travelled. The sound teeth of populations still living on the natural food of their own land contrasted with the rampant decay among the same ethnic groups living on modern foods.
The process whereby easily formentable carbohydrates in the form of refined sugar or refined flour gives rise to acid attack of the tooth enamel is widely agreed as the correct explanation for the history and for the geographical incidence of this destructive disease. The fault is the removal of the carbohydrate from its natural dwelling in plant cells where it invariably exists along with fibre, minerals, vitamins. protein, etc.
If we are to understand the causes of diseases of civilisation it cannot be too often emphasised that our teeth, our digestion and metabolism are evolved to use materials as they occur in nature.T.L. Cleave and Adaptation
Nature's processes are miracles of checks, balances and relationships. Remove those checks and balances and a chain of events is set in motion which may bring our being to a painful and fatal end or to a state of chronic ill health. The perfect and near miraculous adaptation of living creatures to their natural foodstuffs is a constant theme in the writings of T. L. Cleave, an outline of whose theories follows.
Cleave has grouped the diseases by carbohydrate refining under three headings. Firstly, those caused mainly be removal of fibre, secondly by over-consumption and, thirdly, by removal of protein. The three faults are less harmful in 70% extraction refined flour, which is concentrated by some 30%, than in refined sugar which is concentrated by 100% (crystalline sucrose has no trace left of the parent plant).
The two refined carbohydrates of European nations, white flour and sugar, acting alone can do a lot of damage, but when their action is combined the damage is much worse.
By artificially satisfying hunger and blunting appetite a high intake of sugar displaces other carbohydrate foods, thereby lowering the intake of minerals, vitamins and fibre. There is growing agreement that fibre depletion, the main cause of constipation, is therefore responsible for the serious complications of that distressing complaint -- varicose veins, diverticular disease, haemorrholds, appendicitis and large bowel cancer (20). In the case of appendicitis, proliferation of pathogenic bacteria in the bowel lumen, as a result of a high sugar, low residue diet, probably plays a part in aetiology.
In 1979 Cleave was awarded the Harben Gold Medal for his contribution to public health but there are few signs that his work is as widely recognised and acted upon as was the research of previous recipients of that award such as Pasteur, Lister and Fleming. This is particularly true of attempts to prevent coronary heart disease, spokesmen on this subject seldom ever mention Cleave's conception of over-consumption as a cause of the disease nor do they seem to be aware of the history of the extraordinary increase during this century which coronary thrombosis shares with other diseases of civilisation.Over-consumption
Yet over-consumption is surely not difficult to understand even by those unqualified in biological sciences. Sugar, when eaten in its natural setting of cane, root or fruit is relatively slowly absorbed in the human gut. But if it is taken in pure form, particularly as a between-meals snack, the natural check to its quick absorption is removed. To absorb the two or three teaspoonfuls of sugar which might be added to tea or coffee in a between-meal snack it would be necessary to eat four or five apples. So the natural check of appetite satisfaction would prevent the excessively high blood sugar levels which repeatedly occur in those consuming the quantities of refined sugar normal in advanced countries.
Excess glucose (the form in which sugar is ultimately absorbed) is converted to body fat; over-consumption is thus the main cause of the widespread obesity which inevitably occurs in populations eating refined carbohydrates. And with obesity goes diabetes -- sometimes in the same individual -- always in the same population. In its simplest outline Cleave's explanation for the frequent occurrence of late onset diabetes (the commonest type) is exhaustion of the human body's cellular mechanism for dealing with absorbed sugar. Repeated peaks of blood glucose absorbed at unnatural speed overwhelms and wears out the pancreatic insulin-producing cells.Latent Period
The repeated worldwide appearance of diabetes among racial groups as they change from traditional to modern foods cannot be explained without an understanding of the latent period between sugar consumption approaching a certain level and the 'explosion' of the disease.
Cleave has compared the arrival of the per capita consumption of sugar at approximately 100 lb per annum to the lighting of a fuse wire the length of which varies for difierent diseases. Appendicitis explodes immediately. diabetes in 20 years, coronary thrombosis in about 30 years and diverticular disease in 40 years.
As the susceptibilities to disease vary enormously from person to person the diseases do not occur with quite the precision suggested, but the arrival of coronary thrombosis in the Royal Infirmary of Edinburgh as recorded by Dr. Rae Gilchrist (personal communlication) (Table 1) would seem broadly to confirm Cleave's suggestion that the damaged arteries of the coronary patient may simply be due to the exposure of the endothelial lining to repeated high levels of blood glucose.
Table 1. Increasing frequency of cardiac infarction amongst hospital patients at the Royal lnfirmary, Edinburgh (cases recorded by A. R. Gilchrist) Year No. of cases Period (Years) 1924/26 0 2 1928/30 12 2 1939/46 100 7 1947/54 321 7 Fat Consumption and Cholesterol
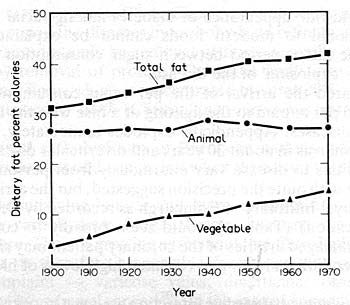
Diabetes is closely associated with small vessel arterial damage and over 50% of mature onset diabetics die of coronary thrombosis (21). We do not know whether the main fault is in the arterial wall or in the circulating blood but we do know that the rise in death rate from coronary thrombosis cannot be related to an increase in animal or saturated fat (22). There has been no rise in consumption of animal fats in Western countries comparable to the huge increase in sugar consumption noted above. Figure 4 shows how in America since 1900 the moderate increase in the consumption of total fat has been due entirely to a rise in the intake of vegetable oils.
Fig. 4. Fat consumption in the United States. (Data provided by Prof. R. E. Olson, St. Louis University).
The cooking oils, shortening, or margarine manufactured from the oil of maize, cotton seeds, soya beans or sunflower seeds cannot qualify as natural foods. Their mass production requires the use of techniques for repeated heating at high temperatures and of solvents, catalysts and various other chemical additives. The relatively higher levels of blood cholesterol in Western nations have for long been regarded as a major risk factor in the cause of coronary heart disease; the purpose of substituting vegetable oils, especially polyunsaturated oil, is to lower levels of blood cholesterol.
When blood cholesterol has been successfully lowered by changes in diet or by drugs no overall reduction in death rate has been demonstrated. Indeed some trials have seemed to show that we lower blood cholesterol at our peril. In the recent WHO sponsored European study (23) on the primary prevention of coronary thrombosis using the drug Clofibrate, blood cholesterol levels were lowered by approximately 9%. This certainly seemed to reduce non-fatal attacks of coronary thrombosis by some 26%, in the experimental group of men taking the drug.
But there was no reduction in fatal heart attacks and an alarming increase of 37% in the treated group in the death rate from causes other than coronary disease. This unfortunate outcome was due to an increase in cancer deaths, particularly cancer of the gastro-intestinal tract. There was an astonishing increase -- more than double -- in the operations for removal of gallstones in the treated group.
In the two primary prevention trials in which diet was used to lower blood cholesterol it seemed death rates from causes other than coronary diseases were higher in the treated group (24).
To the ecologist would not these results suggest that cholesterol may have a protective function in the life of human cells, and that the raised blood cholesterol levels observed in Western societies may be a response to faulty nutrition which has nothing to do with animal fat? There appears to be no constant relationship between the incidence of fatal myocardial infraction and levels of blood cholesterol (25), nor between dietary cholesterol and blood cholesterol. Some statisticians have pointed out that when the effects of sugar consumption and of smoking are taken into account, eggs, meat, milk and saturated fat cease to be a more statistically significant cause of mortality than heart disease (26).Cancer
The increase in cancer death rates following the substitution of unnatural substances in the human diet, be they drugs or artificial foods, suggests that the prevention of cancer may not be quite as baffling as is sometimes suggested.
In a lecture on aastrointestinal diseases in 1922 (27), McCarrison tells how his interest in nutrition was first aroused by observing the outstanding health, fine physique and longevity of certain races in Northern India, particularly the Sikhs and the Hunzas. During a 7-year period as Medical Officer to these people he never encountered a single case of peptic ulcer, appendicitis or cancer.
McCarrison repeatedly emphasIsed the importance of multiple vitamin deficiencies as a cause of lowered resistance to both degenerative and to infective diseases; he was convinced that the high morbidity of the people of Madras when compared with the far healthier population in the Punjab in the North was due to the better nutrition of the latter. Cancer was 3.5 times commoner in Madras. The protective effect of vitamins against cancer seemed to be demonstrated in a laboratory experiment recorded by McCarrison when one of a group of monkeys fed on an experimental diet autoclaved so as to be totally devoid of the B group of vitamins developed an early cancer of the stomach (28).
The count of cases of cancer in a Scottish rural practice (Table 2) gives some idea of the prevalence of this disease in a relatively small population which, as in most rural areas, has an abnormal loading of elderly people. An average of 17 fresh cases of malignancy are diagnosed annually out of a population of some 3400.
About 60% of cases were made up from cancers in three systems; cancer of the bowel and rectum, the largest single group, cancer of the respiratory system and cancer of the male and female reproductive organs. As noted above large bowel cancer may simply be a complication of constipation. Cancer of the male and female reproductive organs may, in my opinion, be related to faulty food through hormone imbalance caused by over-consumption.
Yudkin (29) has demonstrated hyperinsulinism associated with a high sugar intake. His work also suggests a disturbance of adrenal corticol hormone from the same nutritional cause. Eugene Ziegler reviewed international statistics of height and weight and showed that the increase In body stature and the lowering of the age of puberty during the last 150 years in Western nations is closely related to increased sugar consumption (30) . These findings have been confirmed in Northern Canada where Schaeffer (31) noted a marked acceleration of growth and a lowering of the age of puberty in Eskimos living in the trading townships of that region. The growth changes were associated with a fall in the consumption of foods from animal sources and a quadrupling of the intake of sugar.
Table 2. Cancer in a Highland Practice, population 3450, 1975-1981 Total cancers 119 Colon 17 Rectum Bronchus and larynx 17 Male and female reproductive organs, including breast 27 Total 71 Sixty per cent. of all cancers occur in the large bowel, reproductive organs or respiratory system.
In clinical practice sex hormones are often used in an attempt to check the growth of cancer of the breast and prostrate. It seems to me reasonable to suppose their cause may well be hormone imbalance caused by high sugar consumption. This would certainly explain their epidemiology. Steffanson (32 ) found that while they lived on their traditional diet, Eskimos did not suffer from breast cancer which, with other cancers, only appeared among them after years of contact with Western food.
The association between cigarettes and lung cancer has for long been accepted. But Wynn reviewed international statistics of tobacco consumption and death rates from lung cancer and pointed out that death rates from this disease do not constantly relate to tobacco consumption (33). For instance, Scotland has the highest death rate from lung cancer probably in the world (A. Wynn, personal communication) but by no means the highest average tobacco consumption.
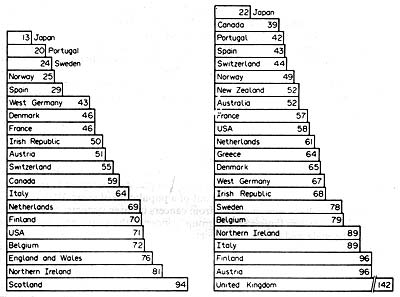
Fig. 5. Death rates of men from lung cancer, aged 45-54. 1973, are shown in the left-hand graph. (Source: WHO, 1973-1976.) Deaths from lung cancer per million lb of tobacco, 1973, are shown in the right-hand graph. (Sources: Lee, 1975, WHO, 1973-1976.) Deaths are per 100,000 men in each age group.
Of the countries listed in Fig 5, left hand column, the Netherlands, Switzerland, West Germany and Japan all consume more tobacco per head of population than U.K., but suffer less from lung cancer. The very high death rate in the U.K. per million tons of tobacco is shown in the right hand column.
The findings suggest that resistance to carcinogens may vary widely between nations and groups within nations. Scots eat less protective foods such as fresh fruit and vegetables than in other parts of the United Kingdom -- probably their intake of these foods is less than in any other part of Europe; instead of fruit and vegetables the Scots eat refined carbohydrates.Thoughts on Prevention
The minutiae of human pathology are infinitely complex, but the basis of health outlined in this paper is simple. The rise and spread of diseases of civilisation in spite of all the amazing advances in medical technology, in spite of all the efficacy of new drugs, and in spite of State fundings of medical care for everyone, is a demonstration of ecological disaster on a vast scale.
Failure by professional leaders and by Governments to grasp the truth of the ecological basis of the diseases of our time finds both Government and profession faced with ever-mounting expenditure on medical care, groping blindly for priorities in prevention. One example of such blindness is the belief that the integrity of our hearts could only be achieved by substituting unnatural polyunsaturated margarine for natural butter. Another example is the proposal, supported by finds from the DHSS, to achieve dental health by dosing the entire population via the water supply with highly toxic compounds of fluorine derived from the waste products of certain industries (34).
Various legislative measures would possibly bring about much needed changes in the production and marketing of food. These might include financial incentives by tax or subsidy to grow and retail food guaranteed free of toxic residues or other additives; similar financial incentives might reduce the consumption of sugar and encourage the retailing of wholewheat bread. A premium on organicaily grown food might allow farmers and market gardeners to employ extra labour without which organic or biological methods are impossible (and incidentally to reduce the number of unemployed).
It is doubtful if the fall in the per capita consumption of sugar in recent decades and the increase in demand for wholewheat bread will yet significantly affect overall morbidity. There appears, however, to be some improvement in dental health in Scotland (35). Unless there is a change in attitude in the medical profession coupled with a change in demand by consumers it is doubtful if present trends will be reversed to affect significantly morbidity from modern diseases.
The attitude of the medical profession is crucial. The broadening of the curriculum in pre-clinical years seems to have done little to give doctors and their leaders a breadth of vision necessary to grasp ecological truths.
The surgeon in his operating theatre doing his appendicectomy is interested only in doing the operation efficiently and well; to him comes satisfaction from thus using his hands to relieve suffering. The techniques of operating absorb all his mental energies. His students are eager to emulate him. Neither surgeon nor students at present appear to be particularly interested in knowing the evidence which strongly suggests that the festering appendix under their hands is the result of a long chain of events determined by man's relationship to his land and its crops. Seldom in the writings of our highly skilled specialists is there a glimmer of the truth that there is a unity in the health of the soil, the health of plants and animals, and of man. The worship of technology finds little time for a comprehension of nature's laws, or for the humility to understand that we cannot defy nature without being punished.
This lecture was first published in "The Ecology of Disease". Vol. 2, No. 1, pp. 81-91 (1983)References
1. D. P. Burkitt. Actiology of appendicitis, Br. J. Surg., 58, 695 (1971).
2. T. L. Cleave. The Saccharine Disease, p. 38. John Wright, Bristol (1974).
3. H. R. Hutt, The geography of cancer, Practitioner. 222, 181 (1979).
4. E. Weiss and E. Spurgeon, Psychosomatic Medicine. Saunders, LondonI
5. H. Selye, The Stress of Life. Longmans Green, London (1957).
6. M. F. Oliver, Does control of risk factors prevent coronary heart disease? Br. Med. J. 28-55, 1065 (1982).
7. G. J. Brisson. Lipids in Human Nutrition, p. 83. M.T. P. Press, London (1982).
8. R. McCarrison, Nutrition and Health. Faber & Faber, London (1953).
9. D. P. Burkitt, Some diseases characteristic of modern western civilisation. Br. Med. J. 1, 274 (1973).
10. J. Thomson, Should modern food carry a health warning? World Medicine 10, 274 (1975).
11. Soil Association Quarterly Review (Winter 1982-83), p. 7. Soil Association Ltd. Stowmarket. Suffolk.
12. K. Miller, Sensitivity to Tartrazine. Br. Med. J., 285, 1597 (1982).
13. W. R. Aykroyd. Sweet Malefactor, p. 1. Heinemann, London (1967).
14. W. R. Aykroyd, Sweet Malefactor, p. 24. Heinemann, London (1967).
15. W. R. Aykroyd. Sweet Malefactor, p. 44. Heinemann. London (1967).
16. J. Yudkin, Pure White and Deadly, The Problem of Sugar. p. 42. Davis Poynter, London (1972).
17. J. C. Drummond and A. Wilbraham, The Englishman's Food. p. 165. Jonathan Cape. London (1957).
18. C. Wells, Bones. Bodies and Diseases, p. 123. Thomas and Hudson, London (1964).
19. W. Price, Nutrition and Physical Degeneration. Hoeber, New York (1939).
20. T. L. Cleave, The Saccharine Disease, p. 107. John Wright, Bristol (1974).
21. L. Michaels, Aetiology of coronary heart disease. An Historical Approach, Br. Heart J. 28, (1966).
22. Committee of Principal Investigators, Br. Heart J. 40, 1069 (1978).
23. Anonymous, Clofiltrate: A final verdict, Lancet 2, 1132 (1978).
24. A. R. P. Walker, Cholesterol and mortality ratios, Br. Med. J. 280, 1320 (1980).
25. C. J. Brisson, Lipids in Human Nutrition. p. 84. M.T.P. Press. London (1982).
26. C. J. Brisson, Lipids in Human Nutrition, p. 83. M.T.P. Press, London (1982).
27. R. McCarrison. Faulty food in relation to gastro intestinal disorder, J. Am. Med. Ass. 79, 1 (1922).
28. R. McCarrison, The Work of Sir Robert McCarrison, p. 198. Faber & Faber, London (1963).
29. J. Yudkin, Pure White and Deadly, The Problem of Sugar, p. 137. Davis Poynter, London (1972).
30. E. Ziegler, Secular changes in the stature of adults and the secular trend of modern sugar consumption, Z. Kinderheilk. 99, 146 (1967).
31. 0. Schaeffer, Pre- and post-natal growth acceleration and increased sugar consumption in Canadian eskimos, Can. Med. Ass. J. 103, 1055 (1970).
32. V. Steffanson, Cancer: Disease of Civilisation. Hill & Wang, New York (1960).
33. M. Wynn and A. Wynn, Prevention of Handicap and Health of Women, p. 87. Routledge & Kegan Paul, London (1979).
34. R. C. P. Report, Fluoride, Teeth and Health. Pitman Medical, London (1976).
35. J. E. Todd, Walker and Dodd, Adult Dental Health, Vol. 2. United Kingdom (1978), HMSO, London (1982).
Medical Testament
The Nature of Health (Introduction and Table of Contents)
Medical Testament
References
McCarrison bibliography (References)
Speeches by Sir Robert McCarrison and Sir Albert Howard
Correspondence in the British Medical Journal
Food and Health -- Lionel Picton
Soil Fertility and Health -- Sir Albert Howard
Soil Fertility: The Farm's Capital -- Sir Bernard Greenwell
Open-Air Dairying -- A.J. Hosier
Farming for Profit with Organic Manures -- Friend Sykes
Nutrition and Health -- Sir Robert McCarrison
Nutrition in Health and Disease -- Sir Robert McCarrison
Studies in Deficiency Disease (Introduction) -- Sir Robert McCarrison
Diseases of Faulty Nutrition -- Sir Robert McCarrison
Nutrition and Physical Degeneration -- Weston A. Price
The Saccharine Disease -- T. L. Cleave
An Agricultural Testament -- Sir Albert Howard
Ill Fares the Land -- Dr. Walter Yellowlees
Food & Health in the Scottish Highlands: Four Lectures from a Rural Practice -- Dr Walter Yellowlees
Back to the Small Farms Library Index
Community development | Rural development
City farms | Organic gardening | Composting | Small farms | Biofuel | Solar box cookers
Trees, soil and water | Seeds of the world | Appropriate technology | Project vehicles
Home | What people are saying about us | About Handmade Projects
Projects | Internet | Schools projects | Sitemap | Site Search | Donations | Contact us